
Prevalence and Causes of Wrong Time Medication Administration Errors: Experience at a Tertiary Care Hospital in Pakistan

by Salimah Taufiq, BscN, MSc Health Informatics
Lead Clinical Analyst EHR Project
Abstract
Purpose: Wrong-time medication administration error (WTMAE) is a high risk to patient safety. It can result in severe harm, death or fatal consequences. Through this study we investigated the prevalence of WTMAEs via electronic medical administration record (eMAR) and explore the contributing factors associated with WTMAEs.
Study design: A descriptive study design with quantitative research approach.
Setting: Data was gathered from a private tertiary care university hospital in Karachi, Pakistan.
Outcome: Determine the prevalence and causes for WTMAEs.
Findings: 250,213 doses were observed, out of which 231,380 (92.5%) doses were administered and 18,833 (7.5%) doses were identified as missed doses. Administered doses (n= 231,380) were further analyzed for on-time administration (n=191,994; 83%) and wrong-time administration (n=39,386; 17%). Study showed high percentage of WTMAE’s during the night shift. Upon further exploration of WTMAEs multiple reasons for late and early medication administration were identified.
Implications: Medication administration is a complex process, and WTMAE is a major area to focus for improving the accuracy of medication administration recording. The study highlights the frequency of WTMAEs and provides opportunities for improvement in nursing practices by elaborating multiple reasons for WTMAEs.
Value: Technology used innovatively in the form of eMAR can significantly help in identifying medication administration errors (MAE). The study also highlights major issues of MAE requiring intervention.
Keywords: Medication errors, Technology, Medication administration.
Introduction
Patient safety issues related to medication administration are critical on a day by day basis. Among all types of clinical errors, medication administration errors (MAEs) are reported as the second most frequent cause of injury. Therefore research needs to be done to identify different types of medication administration errors such as, wrong patient, wrong dose, wrong route, wrong drug, wrong-time and many others. Identification and analysis of MAEs are highly important for process improvement and patient safety. According to Koppel, Wetterneck, Telles, and Karsh (2008) “The Institute of Medicine (IOM) estimates that, on average, a hospitalized patient is subject to one medication administration error (MAEs) per day… In hospitals, the medication administration stage accounts for 26% to 32% of adult patient’s medication errors” (p. 408).
Studies have been conducted to identify MAEs and wrong-time medication administration error (WTMAE) as high risk to patient safety. The National Patient Safety Agency (NPSA) News (2007) reported that WTMAE is the second largest category of medication error reported worldwide and has resulted in death or serious harm to patients. A review of the literature suggested that observational study for wrong time (WT) errors conducted by different methods, showed variation ranging from 10% to 42% at several healthcare institutions (Balas, Scott & Rogers, 2004, Barker, Flynn & Pepper, 2002, Colen, Neef and Schuring, 2003, Prot et al., 2005). In addition Fitzhenry et al., (2007) reported wide disparity in wrong-time error rates, ranging from 0.5% to 35.7%. He defined WT errors as “dose administered > 60 minutes before or after scheduled time” (p.760). Khowaja et al., (2008) highlighted that 26.4% of medication errors are due to delayed dispensation of drug from pharmacy. Allan and Barker (1990) suggested that wrong-time errors were defined as deviations from hospital policy.
The purpose of this study was to investigate the prevalence of WTMAE with the help of technology and to explore factors contributing to WTMAE. This study compared actual versus expected medication administration time, captured from an electronic medication administration recording system (eMAR). The study was conducted at a tertiary care hospital in Pakistan where the electronic medication administration record (eMAR) was used at all inpatient locations. The study findings provide an opportunity to decrease patient care risk and assist in development of different strategies for system improvement to ensure safe practices.
Literature review
A literature review was done using different search engines such as Pub-Med, EBSCO host CINAHL Plus and Cochrane Database of Systematic Reviews. Attempts were made to find the literature from the primary source library and some of the literature was explored through secondary sources (University of Sheffield) library.All electronic databases were searched for references with key terms such as medication error, medication administration error and wrong-time medication administration errors. The search was limited to literature available from January 2000 to December 2011. Pub-Med search revealed 1642 articles, EBSCO host CINAHL Plus provided 220 and the Cochrane database revealed 1551 full text articles with search term: “medication error”. The search was narrowed to search term “wrong-time medication administration error” which revealed limited full text articles. Leading studies are summarized in Table I.
Table I: International studies on medication administration errors
Methodology
Study Design
A quantitative descriptive study design was used. Data for this study was gathered through the eMAR system, which identified the dose timing (actual verses expected) with reasons for early or late administration.
Setting
The study was conducted at a private tertiary care university hospital in Karachi, Pakistan. It serves over 600,000 out-patients and 50,000 inpatients annually. This study included five in-patient locations; i.e., medical, surgical, coronary care, intensive care and pediatric units (37% of total inpatient beds). These units were chosen to cover most of the specialty areas for adult and pediatric patients with medical and surgical conditions. Approval for data collection was requested from relevant departmental heads and the hospital Ethical Review cCmmittee (ERC).
Sampling
A universal sampling technique was used to capture all the medication doses prescribed for the 3-month period from February 10, 2012 to May 9, 2012. This activity was initiated only after getting approval from hospital departmental heads and the ERC.
Data collection
The data for this study was gathered through the eMAR system from designated locations. All medication administered daily from 00:00 hours to 23:59 hours for 3 consecutive months were included in the study. The information was then exported to Microsoft Excel for analysis.
Data analysis
Data received from the eMAR was coded for different variables and analyzed in SPSS version 19. Additionally Chi-square test was used to analyze data for differences between wrong-time administration verses on-time administration at different locations and shifts, to identify any significance difference. Lastly data was analyzed to identify the reasons for any WTMAEs.
Results
The results illustrate that, overall 250,213 doses were prescribed for all of the five selected inpatient locations during the study period of 90 days. The finding indicates that out of 250,213 prescribed doses 231,380 doses were administered whereas 18,833 doses were not administered (see Table 2).
Table 2: Prescribed, administered and missed doses

Subsequently data from the total number of administered doses (n=231,380; 100%) were analyzed to obtain the on-time administrated doses (n= 191,994; 83.0%) and wrong-time administrated doses (n=39,386; 17.0%). The data showed 17% prevalence of WTMAEs at the tertiary care university hospital in Karachi, Pakistan. Findings of this analysis are presented in Figure 1.
Figure 1: On-time verses wrong-time doses
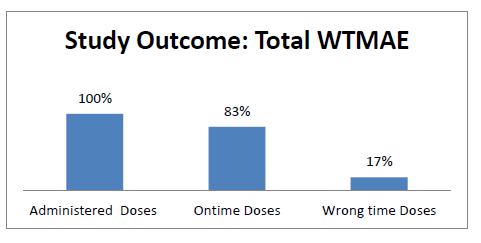
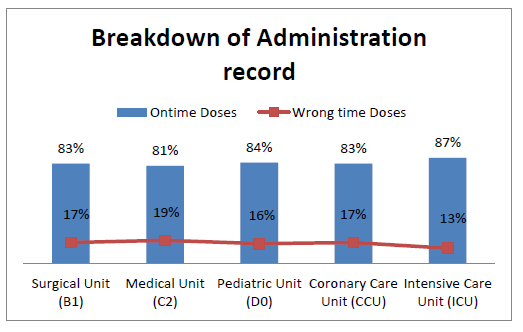
Figure 2 summarizes the percentage of on-time and wrong-time medication administration record by locations.
Figure 2: On-time and wrong-time medication administration record by different locations
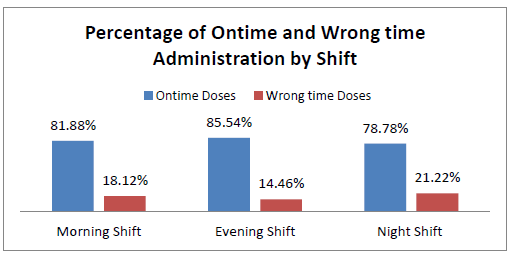
Data was also analyzed to measure WTMAEs in different shifts to identify the impact of shifts on WT errors. This hospital has nursing staff working three eight hour shifts. The highest number of medication administration was reported in the evening shift; whereas the highest percentage of WT administrations was reported in the night shift; i.e., 21.22% (see Figure 3).
Figure 3: On-time and wrong-time medication administration by shift
The eMAR system was programed to allow nurses to administer a medication dose 60 minutes prior or later to its scheduled time only after giving a short reason. This systemic intervention helped us to identify many reasons for early or late medication administration errors. These reasons were further grouped to list 35 reasons (Table 3) for late administration and eight reasons (Table 4) for early administration. Figures 4 and 5 depict the top five reasons for late and top three reasons of early administration.
Figure 4: Early administration – main reasons
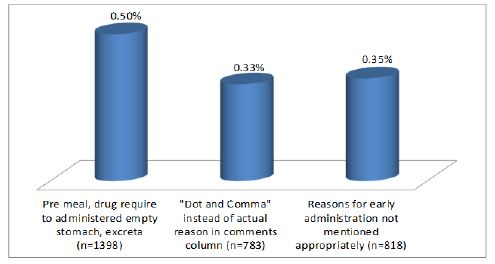
Figure 5: Delayed administration – main reasons

Table 3: Reasons for delayed medication administration
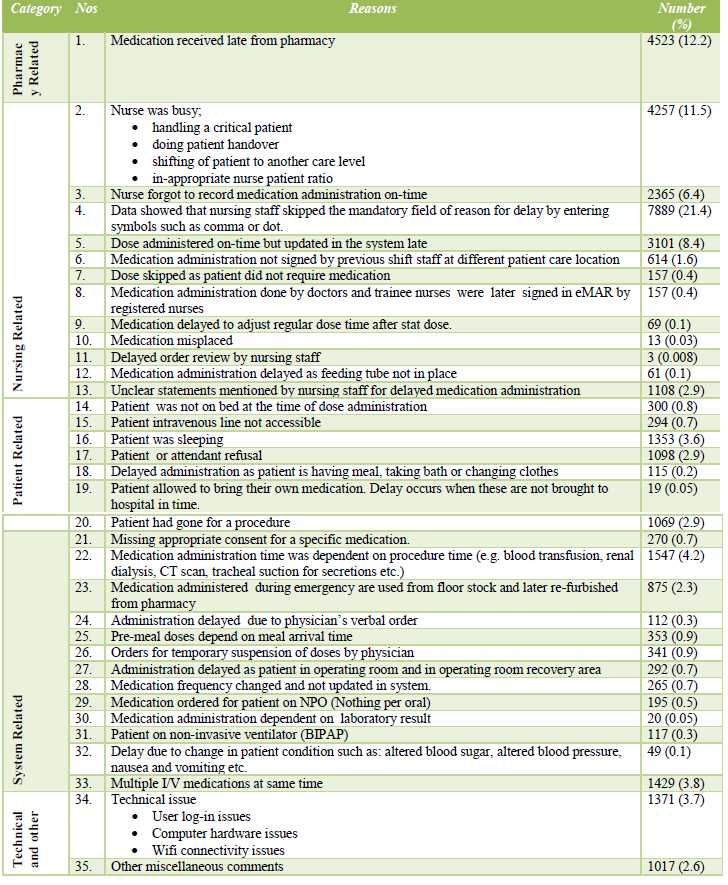
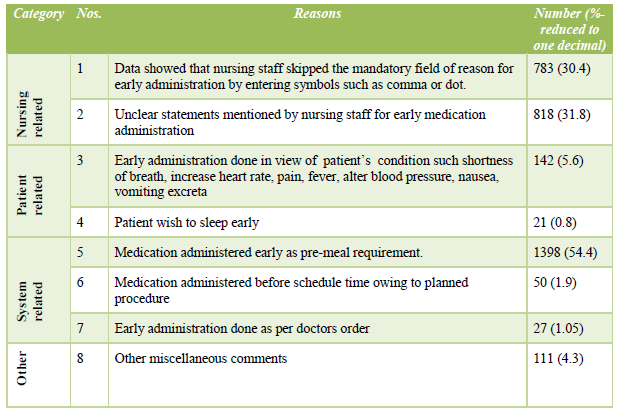
Table 4: Reasons for early medication administration
Discussion
The data on WT medication administration errors illustrates that error identification from electronic system helps to give accurate number of errors and avoid any Hawthorne effects on the study; whereas the literature search revealed that most of the previous studies used observational methods to gather medication administration error data (Bates,. 2000). Our study results showed a total of (n=39,386; 17%) doses in error due to WT administration in a three month period. The data also displayed how timing errors are not considered a major issue and have been given less attention. It has been mentioned by Fitzhenry et al., (2007) that“the effects of timing errors and errors of omission were rarely recognized clinically” (p. 762). Our study is the first from a third world country showing 17% WTMAE. Many studies conducted internationally on medication errors presented WTMAE in ranges from 3% to 45% (Bemt et al., 2007; Szczepura et al., 2011).
Conclusion
Medication administration is a complex process. The most important contribution of this study was the focus on wrong-time medication administration errors and their contributing factors. The study shows that innovative technology and its role in identification of MAE and WTMAE are imperative and well supported by the literature. Electronic medication administration record systems act as a great tool to capture the administration record in a timely manner and to help to correctly estimate the prevalence of WTMAE and the reasons behind the wrong-time administration.
Recommendations
Available literature on WTMAEs via electronic data bases is limited. International studies conducted on wrong time error were reported using observational and chat review methods via manual medication administration record. Conducting a study in a developing nation through eMAR is a new experience. This study’s finding suggest that staff members ought to be sensitized to the importance of on-time medication administration, which requires strong enforcement by management in the form of institutional policy. Also regular audits of medication administration records in the eMAR should be done to check for WTMAE. The senior management must also be apprised of the fact that to create a culture of patient safety, correct nurse-patient ratios are important to curtail WTMAE.
References
Allan, E. L. and Barker, K.N. (1990), Fundamentals of medication error research, American Journal of Hospital Pharmacy, 47 (3), p. 555-71.
Balas, M.C., Scott, L.D. and Rogers, A.E. (2004), ‘The prevalence and nature of errors reported by hospital staff nurses’, Applied Nursing Research, 17 (4), p. 224-230.
Barker, K.N., Flynn, E. A. and Pepper, G.A. (2002), ‘Observation method of detecting medication errors’, American Journal of Health System Pharmacy, 59 (23), p. 2314-6.
Barker, K. N., Flynn, E. A., Pepper, G.A., Bates, D.W. and Mikeal, R.L. (2002), Medication errors observed in 36 health care facilities, Arch Intern Med, 162 (16), p. 1897-903.
Bates, D. W. (2000), Using information technology to reduce rates of medication errors in hospitals, British Medical Journal, 320 (7237), p. 788-91.
Bemt, V.D., Robertz, R., DeJong, A.L., Van Roon, E.N. and Leufkens, H.G.M. (2007), Drug administration errors in an institution for individuals with intellectual disability: an observational study, Journal of Intellectual Disability Research, 51 (7), p. 528-536.
Bemt, V.D., Fijn, R., Van Voort, P.H.J., Gossen, A.A., Egberts, T.C.G. and Brouwer, J.R.B.J. (2002), Frequency and determinants of drug administration errors in the intensive care unit, Critical Care Medicine, 30 (4). p. 846-50.
Buckley, M. S., Erstad, B. L., Kopp, B.J., Theodorou, A.A. and Priestley, G. (2007), Direct observation approach for detecting medication errors and adverse drug events in a pediatric intensive care unit, Pediatric Critical Care Medicine, 8 (2), p. 145-52.
Calabrese, A. D., Erstad, B. L., Brandl, K., Barletta, J.F., Kane, S.L. and Sherman, D.S. (2001), Medication administration errors in adult patients in the ICU Intensive Care Medicine, 27 (10), p. 1592-8.
Colen, H.B., Neef, C. and Schuring, R.W. (2003), ‘Identification and Verification of Critical Performance Dimensions: Phase I of the Systematic Process Redesign of Drug Distribution’, Pharmacy World Science, 25 (3), p. 118-125.
DeYoung, J.L., Vanderkooi, M.E. and Barletta, J.F. (2009), Effect of bar-code-assisted medication administration on medication error rates in an adult medical intensive care unit, American Journal of Health System Pharmacy, 66 (12), p. 1110-5.
FitzHenry, F., Peterson, J.F., Arrieta, M., Waitman, L.R., Schildcrout, J.S. and Miller, R.A. (2007), Medication Administration Discrepancies Persist Despite Electronic Ordering, Journal of the American Medical Informatics Association, 14 (6), p. 756-764.
Khowaja, K., Nizar, R., Merchant, R.J., Dias, J., Bustamante, G.I. and Malik, A. (2008), A systematic approach of tracking and reporting medication errors at a tertiary care university hospital, Karachi, Pakistan, Therapeutic Clinical Risk Management, 4 (4), p. 673-9.
Koppel, R., Wetterneck, T., Telles, J.L. and Karsh, B.T. (2008), ‘Workarounds to Barcode Medication Administration Systems: Their Occurrences, Causes, and Threats to Patient Safety’, American Medical Informatics Association, 15(4), p. 408-423.
Michael, R. (2007), ‘Information System: Paper-based MARs Marred with Inefficiency. Extended Care Product News-ISSN’. 123 (9): 43-44 National Patient safety Agency (2010). Safety in Doses. Improving the use of medicines in the NHS 2009. NPSA, 2007. http://www.nrls.npsa.nhs.uk/resources/?entryid45=61625
Nelson, N.C., Evens, R.S., Matthew, H.S. and Gardner, R.M. (2005), Detection and Prevention of Medication Errors Using Real-Time Bedside Nurse Charting, Journal of the American Medical Informatics Association, 12 (4), p. 390–397.
Prot, S., Fontan, J.E., Albert, C., Bourdon, O., Farnoux, C., Macher, M.A., Foureau, A., Faye, A.,Beaufils, F., Gottot, S. and Brion, F. (2005), ‘Drug administration errors and their determinants in pediatric in-patients’, Internal Journal of Quality Health Care, 17 (4), 381-389.
Szczephra, A., Wild, D. and Nelson, S. (2011), ‘Medication administration errors for older people in long-term residential care’ BioMed Central Geriatric, 11 (82), p. 1471-1480.
Tissot, E., Cornette, C., Limat, S., Mourand, J.L., Becker, M., Etievent, J.P., Dupond, J.L., Jacquet, M. and Woronoff-Lemsi, M.C. (2003), Observational study of potential risk factors of medication administration errors, Pharmacy World Science, 25 (6), p. 264-268.
About the Author
Salimah Taufiq Kirmani BScN, MSc Health Informatics
As a System Analyst, I am involved in the planning, development and implementation of different clinical systems to enhance technology in nurses. Currently work as a Lead Analyst Nurse working with EHR Core Committee for selection of suitable software for Electronic Health Record for all the Aga Khan Hospitals in Asia & Africa.
Acknowledgement
Professor Peter Bath
Professor of Health Informatics
BSc (Technical) (University of Wales), MSc (Sheffield), PhD (Sheffield)
My special thanks to my supervisor Dr. Peter Bath, for his ongoing encouragement and continued guidance.




Recent articles
- Index of volume 21 number 221 Jun 2026
- What does Canada’s new National Artificial Intelligence Strategy mean for healthcare?21 Jun 2026
- UN SDGs and Open Source Principles as Outcomes and Implementation Approach to Health Informatics21 Jun 2026
- Designing Compassionate Systems: Why Nursing Must Lead in the Age of AI21 Jun 2026
- Advancing Nursing Informatics Through the Integration of Genomics: Addressing Barriers and Capacity Building in Canadian Healthcare21 Jun 2026