
Nursing’s Voice in Healthcare IT Acquisition Decisions

By Allen McLean, RN MN MSc PhD(c),
University of Saskatchewan)
Noreen Frisch, PhD RN FAAN
(Professor, University of Victoria)
Abdul Roudsari, PhD
(Professor, University of Victoria)
Abstract
 Background: The participation of senior nursing healthcare executives in the acquisition of electronic healthcare information systems is not well understood. This is an important issue because nurses make up the majority of care-providers within the Canadian healthcare system, and thus the majority of the information systems end-users. End-user involvement in the selection and evaluation of a healthcare information system is vital to implementation success. The purpose of this study was to explore this gap in our understanding, to find ‘Nursing’s Voice’ in the acquisition and evaluation process.
Background: The participation of senior nursing healthcare executives in the acquisition of electronic healthcare information systems is not well understood. This is an important issue because nurses make up the majority of care-providers within the Canadian healthcare system, and thus the majority of the information systems end-users. End-user involvement in the selection and evaluation of a healthcare information system is vital to implementation success. The purpose of this study was to explore this gap in our understanding, to find ‘Nursing’s Voice’ in the acquisition and evaluation process.
Method: A quantitative study was developed in two parts; nursing informatics experts from across Canada were recruited to evaluate and comment on the study questionnaire, then senior healthcare executives with a background in nursing from each of the health authorities across British Columbia were recruited to participate in an online survey. An N=11 of senior nursing executives were invited to participate, and a response rate of 82% was achieved.
Findings: Most significantly, the respondents indicated a strong interest and desire to participate in hospital informatics projects. The respondents indicated they were often invited to join a project team, generally felt welcomed by the hospital IT staff, felt they made an important or significant contribution, developed knowledge and skills on-the-job and through personal study, and feel nurses should always be included when clinical IT projects are planned.
Conclusion: The results showed that despite a lack of formal training in information technology subjects, the majority of these nursing leaders do take an active role in electronic healthcare information systems acquisition and upgrading projects along-side their health informatics and IT colleagues. The results specific to this research indicate ‘Nursing’s Voice’ is clearly heard.
Keywords
Nursing, Nurse Executives, Nursing Leadership, Electronic Healthcare Information Systems, Acquisition, Evaluation, Participation, Quantitative, Survey, British Columbia, Health Authority
Introduction
“Software innovation, like almost every other kind of innovation, requires the ability to collaborate and share ideas with other people, and to sit down and talk with customers and get their feedback and understand their needs.” – Bill Gates (The Guardian, 2014).
The construction of any software system is an innovative endeavour, and an electronic information system is often a complex software system innovation. The Canadian healthcare system is vastly complicated at every level. Placing a complex software system into a complex healthcare system is rife with the possibility for failure. Senior healthcare executives have an invaluable role to play in maximizing the potential for successful implementation.
The process of acquiring or upgrading an electronic information systems includes an initial investigation, systems analysis, iterations of design, system implementation, and finally, on-going maintenance. This process is often referred to as the ‘Systems Development Life-Cycle’ (SDLC). User involvement in the SDLC process is an accepted, and now preferred strategy when planning for the installation of a new or upgraded information system (Larman, 2005).
Background
Nurses are the largest group of regulated health professionals in Canada. As of 2011, there were 268,512 registered nurses (RNs), 81,224 licensed practical nurses (LPNs), and 5,174 registered psychiatric nurses (RPNs) working in Canada. In all, there are 354,910 regulated nurses working as nurses in Canada (Canadian Federation of Nurses Unions, 2011). To put this in perspective, in 2010 just over 1,000,000 individuals worked directly in healthcare occupations in Canada. For every 100,000 Canadians, there were 780 registered nurses, 190 physicians, 58 dentists, 49 physiotherapists, and 2 midwives (Healthcare Quarterly, 2010).
Electronic healthcare information (EHI) systems of all types are becoming more and more prevalent in the Canadian healthcare system, and in a wide variety of practice settings (Canada Health Infoway, 2013). One research study, published in 2011, showed that 92% of the recent articles on health information technology reached conclusions that were positive overall. In this same study, researchers also found that the benefits of the technology are beginning to emerge in smaller practices and organizations, benefits already seen in large organizations that were early adopters (Buntin, Burke, Hoaglin, & Blumenthal, 2011). A second paper, published in 2013, commissioned by Canada Health Infoway, concluded that the increased use of electronic health record systems helped reduce costs in Canada’s healthcare system by approximately 1.3 billion Canadian dollars over six years (PricewaterhouseCoopers, 2013).
The movement away from paper-based systems to electronic ones is an accelerating and permanent shift in the way we manage information in the Canadian healthcare system. Because nurses are such an integral part of the Canadian healthcare system, and because all signs demonstrate that the Canadian healthcare system is adopting EHI systems, it is logical to conclude that Canadian nurses should play a role in the initial evaluation and acquisition of new or upgraded EHI systems in their workplaces. Do educators and experts agree?
The University of Victoria has recognized the importance of nursing’s role in health informatics. Respected and well-known faculty from the schools of nursing and health information science have developed a novel, first of its kind double-degree master’s program in nursing and health informatics. “Such competencies are essential for professionals working in the rapidly expanding fields of nursing and health informatics. There is an immediate and longer-term need for clinical professionals with such expertise in Canada. Furthermore, a program was needed to provide graduate level credentialing in nursing and health informatics so graduate students could develop needed workplace competencies at the intersection of nursing and health informatics in the international move towards electronic health records.” (Borycki, Frisch, McIntyre, & Kushniruk, 2011). Well-respected experts in the USA have made similar recommendations, including Dr. William Hersh, a leader in health informatics teaching and research from the Oregon Health & Science University, (Hersh, 2009) and Dr. Suzanne Bakken, RN, a leader in nursing informatics research and education with Columbia University (Yale University School of Nursing, 2011).
Rationale
But why should senior nurse executives and leaders develop expertise in IT acquisition, upgrading and evaluation? Aside from better assuring implementation success as mentioned, nurse executives and leaders are responsible for a workforce that must provide safe and efficient care in a complex sociotechnical environment. Quality measures at the provincial and national level rely on information technologies to provide data collection, shared information, and analytic capabilities to inform approaches to care that have the potential to achieve better outcomes. As a key member of the quality assurance team, the senior nurse executives and leaders must provide the infrastructure to build and manage nursing knowledge and instill accountability for following evidence-based practices (American Organization of Nurse Executives [AONE], 2009). Providing this infrastructure will contribute to the so-called ‘learning health system’, where new knowledge is captured as a by-product of care delivery, enabled by knowledge-based electronic systems. The learning health system also relies on rigorous scientific evidence embedded into practice at the point of care. The nurse executive must have the knowledge to be able to optimize the use of knowledge and information-based technologies, integrated throughout the organization (Cipriano, 2012).
Some might argue that the acquisition and evaluation of EHI systems is outside the scope of a nurse’s professional practice, and that these decisions are best left to the Information and Communications Technology (ICT) experts employed in most Canadian healthcare institutions. At first glance, this position does seem to make sense; allow the clinicians to do their clinical work, and allow the healthcare ICT experts to support that work with appropriate and well-designed EHI systems. However, as previously mentioned there is growing acceptance that end-users should be involved in the information systems development life-cycle if successful implementation is to be optimized. User involvement offers many benefits; the development of a rich and grounded understanding of the issues, an opportunity to build community capacity, the fostering of stakeholder cooperation, facilitated data collection, the increased likelihood of project success, reduced costs to the system, and empowering community self-guidance, to name only a few (Kung, 2013).
Nurses make up the majority of healthcare professionals in the Canadian healthcare system. As such, nurses are also the largest group of electronic information systems users, and it would therefore seem appropriate and logical that nurses, or at a minimum their leadership, would have a voice in the selection and implementation of new or upgraded EHI systems. Decisions concerning the acquisition or upgrading of an EHI system take place at the highest levels of healthcare administration, usually involving a provincial government (Canada) and the senior executive team in each health region or authority. Generally speaking, these teams include individuals with a nursing background, however little is known about the participation of senior Canadian nursing executives and leaders when a decision is made to acquire or upgrade an EHI system. Where is ‘Nursing’s Voice’ in EHI systems acquisition? The purpose of this research study was to explore this gap in our understanding.
Literature Review
Please note that due to practical constraints, only the more significant results of the literature review are included in this manuscript. The complete research paper, the authors MN/MSc thesis, may be viewed at https://dspace.library.uvic.ca/handle/1828/5757.
Specific Literature
No published research in respected peer-reviewed journals directly addressing the question of senior nursing executives’ participation in EHI systems acquisitions could be found in the literature. A systematic search of the appropriate academic databases was completed during 2014. This search was completed in the English language, and extended back through 2004.
Background Literature
Despite this lack of published research directly addressing the key questions, there are many professional guidelines and opinion pieces (grey literature) written on the importance of nurses’ involvement in EHI systems projects. There are also some research articles on the topic of nurse executives and informatics. This background literature fell primarily into 2 categories; recommendations concerning the roles and responsibilities nurse executives should embrace within healthcare IT, and recommendations concerning the development of needed health IT competencies amongst nurse executives.
Roles and Responsibilities
The American Organization of Nurse Executives (AONE) have published several guidelines stressing the importance of nursing leadership involvement in electronic healthcare information systems acquisition and evaluation decisions, and were in fact one of the first organizations to publish such guidelines. AONE guidelines from 2012 stress the importance of interdisciplinary cooperation when acquiring an EHI system. The AONE recognized that technology would be crucial to the health care environment of the future, and that successful implementation would be determined by positive collaborations between the departments of clinical information technology and nursing. The AONE argues that each stakeholder has a perspective on how they perform their work; however, they don’t always share these perspectives. One recommended starting point is to clearly articulate their varied perspectives in an effort to increase mutual understanding and appreciation of their differing goals and challenges (AONE, 2012).
AONE guidelines from 2010 are perhaps the most relevant to consider in this research. The AONE firmly believes that the chief nurse executive (CNE) should play a critical role in the selection and implementation of information systems. Acquiring new systems is a complicated process that impacts the entire facility. Although some tasks may be delegated, the chief nursing officer must remain actively involved in the overall decision-making and implementation process, a view shared by this researcher as critical for project success. These guidelines from the AONE reflect a strong belief in the nurse executives’ involvement in the entire SDLC when acquiring or upgrading an EHI system, a position shared by the researchers in this study. So it must be asked, do we share similar beliefs and guidelines here in Canada? The Academy of Canadian Executive Nurses (ACEN) has published some guidelines on this subject, but they are quite broad and do not specifically go into the level of detail the AONE has in their guidelines (Academy of Canadian Executive Nurses, 2011).
Related literature focuses on the importance of strong relationships between clinical and technical hospital staff. In an interesting piece, written from a different perspective by an experienced Chief Nursing Officer (CNO) titled “The CNO and “techies”: A dynamic duo”, (Beard, 2006): this CNO argued that clinical nursing staff often undervalue the role of the IT department. This is not uncommon in healthcare, where clinical staff are often held in higher esteem. The author argues that nurses should be encouraged to approach information technology staff members with an attitude that recognizes the important skills they bring to the organization. Health informatics professionals are an integral part of each healthcare facility and without their skills modern healthcare could not function. Health information science professionals frequently accomplish tasks that are invisible to the majority of us, but have a constant impact on the delivery of care. This opinion is well argued, and strengthens the view that healthcare IT projects succeed based partly on strong multi-disciplinary cooperation and involvement, a key theme of this research. Additionally, nurses have played an increasingly important role in the SDLC, though typically as employees within the various medical software vendors, usually in sales and training (Thede, 2008).
Informatics Competencies
The development of informatics competencies among nurse executives is the second substantive area within the background literature search. ‘Innovation in transformative nursing leadership: Nursing informatics competencies and roles’ focuses on an emerging “avant-garde executive leadership competency”, recommended for today’s health leaders in guiding health system transformations. Specifically, this competency is articulated as “state of the art communication and technology savvy,” (Remus, & Kennedy, 2012, p. 14) and it implies linkages between nursing informatics competencies and transformational leadership roles for nurse executives. The authors of this powerful paper, nursing informatics experts Remus and Kennedy argue that “distinct nursing informatics competencies are required to augment traditional executive skills to support transformational outcomes of safe, integrated, high-quality care delivery through knowledge-driven care. International trends involving nursing informatics competencies and the evolution of new corporate informatics roles, such as chief nursing informatics officers (CNIOs), are demonstrating value and advanced transformational leadership as nursing executive roles that are informed by clinical data” (p. 14).
Many leading healthcare organizations within and outside Canada have also contributed their ideas regarding nursing competencies in health informatics; these include the Canadian Association of Schools of Nursing (Canadian Association of Schools of Nursing, 2012), COACH (COACH, 2012), the Health Information Management and Systems Society (Health Information Management and Systems Society, 2012), and the Canadian Nurses Association (Canadian Nurses Association, 2006), to name only a few; all stress the importance of both involvement and education. These guidelines and recommendations all share many common recommendations, and all encourage nurse executives’ participation in healthcare IT projects.
Literature Summary
On a final note, a 2013 paper in the journal ‘Nursing Management’, (Procter, Hayward, Heyes, & Owen, 2013) summed up nicely why it is important that nursing leaders embrace informatics, and the pivotal role(s) they might occupy within this still emerging discipline. Authors from nursing and health informatics backgrounds worked collaboratively in publishing this paper. They argue that “information and communication technologies are increasing the availability of health care, and improving the management, sharing and understanding of health care, at a local and national level. Senior nurse leaders are in a prime position to interpret data held by healthcare organisations, and act on it to plan, deliver and evaluate service provision to support patient-centred care. Nursing is at the centre of patient-centred care and, as such, draws together effective care across many domains, thereby making nurses ideally equipped for fulfilling the role of Chief Clinical Information Officer (CCIO)” (p. 26). The focus on tying clinical care and outcomes, with the provision of healthcare IT services is fundamental to nursing informatics, and a strong reason to support the presence of ‘Nursing’s Voice’ in healthcare IT projects. Financial decisions, selection decisions, and evaluation decisions are only a few of the recommended areas where senior nurse executives should be involved.
Methodology
Both the survey and interview method were considered to be the best options for this project, and both could have been used to address the problem statement and research questions. The survey method was selected because nurse leaders are typically very busy, and a survey taken at their own convenience should encourage and increase participation; an interview could be seen as too much of a commitment, too invasive, lacking confidentiality, leading to inadequate participation, resulting in meaningless or non-generalizable results. A survey methodology can provide needed structure to the research process, ensures a consistent approach, and offers the opportunity to perform descriptive statistical analysis (LoBiondo-Wood & Haber, 2010).
Development of Study Instrument and Pilot Testing
Researchers have the choice of selecting an instrument that has been previously designed and tested, or constructing a new instrument for their study. Developing a new instrument that is valid and reliable can be both a time-consuming and costly undertaking; it is worthwhile undertaking an in-depth review of the literature to identify if a suitable tool is available (Kasunic, 2005). A suitable survey questionnaire could not be found and therefore a unique instrument was developed. The survey questionnaire looked at the participants demographics (nursing background, years of experience, education attained), their informatics experiences (participation in selection, evaluation, and financial decisions), and their attitudes towards informatics (involvement, feelings of acceptance on the IT team, desire to be involved in the future). The questions asked were chosen based on the recommendations of nursing informatics experts, the literature review, and practical constraints.
Pilot-testing with expert informatics nurses should ensure the instrument is both valid (that it measures what it is designed to measure) and reliable (that it is consistent in that measurement). Failure to achieve validity and reliability can lead to measurement errors where the participant responses do not relate to the research question, are open to misinterpretation, or there is no homogeneity when compared to other participants responses (Coughlan, Cronin, & Ryan, 2009). Before administering a data gathering instrument it is important to evaluate its internal validity and reliability. This is particularly the case when it is a newly developed questionnaire or where a previously tested questionnaire is to be used with a different cultural group or environment. Experts recommend submitting the questionnaire to both subject area experts and to experts in survey design to test both content and design validity. Practical constraints limited our pre-testing solely to subject matter experts, all of whom offered useful insights into potential difficulties encountered by respondents, and their views on the format and language of the instrument.
Study Design
The study design was divided into two main steps; first the development and validation of the study instrument with nursing informatics experts (asking for feedback on the initial survey questionnaire), and second, the invitation to participate in the study sent to senior nursing executives. These steps were sequential with no chronological over-lap.
Study Sample
The research consisted of two groups; respected and established nursing informatics experts from across Canada (NIEs), and senior nurse executives (SNEs) and leaders employed at the highest levels of management in Health Authorities within British Columbia. Both of these samples can be considered convenience samples, but because of the common characteristics shared by individuals working in nursing informatics research (NIEs), and nurses working within senior leadership teams (SNEs), population representativeness should be maintained (Jackson & Verberg, 2007).
NIEs: There are only a handful of nursing informatics experts in Canada, typically employed within universities and colleges, or provincial and national organizations. Five responses were considered adequate by the research team to satisfy the requirements of the first stage of this project, and this number was confirmed in the literature (Jackson & Verberg, 2007). The nursing informatics experts were selected based on their reputation and current activity within the nursing informatics community. Each expert invited to participate in this study was employed in a Canadian university or college, has an active teaching role, has recent publications in nursing informatics, and are members of nursing informatics associations in some capacity. A total of five nursing informatics experts were contacted and invited to participate, and all generously agreed.
SNEs: The acquisition and evaluation of electronic healthcare information systems is very complex, and typically very expensive. These types of decisions are made at the highest levels of administration, usually between senior executives in provincial governments and regional health authorities. There are 7 Health Authorities across British Columbia; a total of 82 senior healthcare executives were identified, 14 having a nursing (RN) background.
Sample Size
This study is limited in this regard; the sample populations of interest in both groups is very small. As might be expected, the number of senior healthcare executives in British Columbia is already a small group, and adding the requirement of a nursing background further limited the potential sample size. There are very few individuals meeting the inclusion criteria for this project, from both groups.
When thinking of generalizability, in this context we are asking if the results can be extrapolated to senior nursing executives in other provinces, and this often depends on whether participants were selected for the study by means of random sampling techniques (Jackson & Verberg, 2007). Study results based on random samples are considered generalizable, if adequate responses were received. This study did not use random sampling techniques; it would have been unfeasible considering the very small number of individuals meeting the inclusion criteria. If the targeted population is a small subpopulation within a larger population, the results may not be generalizable to the larger population. Other information is needed to establish generalizability. Inclusion and exclusion criteria help identify the population to which the results might apply. By carefully examining the characteristics of the study participants, readers can make their own judgements as to the similarities to their own populations of interest.
Data Collection
This research was conducted using the FluidSurveys (FluidSurveys, 2014) website that was generously loaned to the PI by the leadership team at InspireNet (InspireNet, 2014). Data received from the respondents was loaded directly to spread sheets reducing both time and the risk of error while ensuring anonymity and confidentiality. The NIEs received an invitation to provide survey questionnaire feedback on the original survey questions. The SNEs received an invitation to participate which included a link to the online, self-administered survey questionnaire. This link connected the senior nurse executive to the FluidSurveys website, and the survey questionnaire. All data was removed from the website after the survey was closed.
Data Analysis
A survey questionnaire easily permits the reporting of descriptive statistics. The demographic data collected allows for the comparison of experiences across Health Authorities, practice settings, and other variables. Demographic data was compared, as well as information derived from the questions asked in the survey questionnaire. Finally, a summary of themes from the structured short answer questions was reported in a narrative format. Because this research is in the exploratory stage, and the design simple, basic descriptive statistics will be used to report and interpret results. Tests of significance are not appropriately applied in this research study (Bennett et. al., 2011).
Ethical Considerations
Issues of privacy, confidentially, the proper recruitment of participants, and data integrity are taken very seriously by these researchers. Two important ethical considerations of particular relevance in this study relate to informed consent and confidentiality. The respondents were informed of the purpose of the study, their right to refuse to participate and, their ability to withdraw from the study at any time with no consequences. Potential participants were also informed that their identities were anonymous, and the data kept confidential. In the case of questionnaires, consent is usually regarded as implicit in the completion and return of the questionnaire, (LoBiondo-Wood & Haber, 2010) as in this study.
Results
Please note that due to practical constraints, only the more significant research results are included in this manuscript. The complete research paper, the authors MN/MSc thesis, may be viewed at https://dspace.library.uvic.ca/handle/1828/5757.
Step 1: Survey Pilot-Testing
All NIEs provided feedback on an original survey questionnaire; there was substantial differences in both the breadth and depth of the recommendations between the various experts. Much of the feedback was incorporated into developing the final version of the survey questionnaire, though not all the recommendations could be practically accommodated. Regardless, almost all of the feedback was adopted, and the contributions of the nurse informatics experts who selflessly volunteered their valuable time is greatly appreciated.
Step 2: Research Study
The recruitment of SNEs from Health Authorities across British Columbia was begun only after an improved and approved survey questionnaire was completed. Their participation in this work, by generously donating their time and completing the modified survey questionnaire, is greatly appreciated.
Response Rate
The survey questionnaire was open on the FluidSurveys website between September 1 and 15 of 2014 inclusive, which was judged a reasonable amount of time. Based on the fact that all Health Authorities in British Columbia provide detailed information on their senior executive teams online, the PI was able to quickly and easily identify all the senior healthcare executives in BC health regions with an appropriate nursing background. An N=14 was established, and invitations were sent to the 14 qualifying senior healthcare executives with nursing backgrounds as described in the study sample inclusion criteria. Of those 14, one was excluded immediately because she had retired one month before the invitation to participate was sent out, and two were excluded after the PI received ‘out-of-office’ automated email responses confirming that these two executives would be away during the time the survey was live. These two were then also excluded from the sample of interest leaving a total of 11 potential respondents. The study received a total of nine completed survey questionnaires, a respectable 82% response and 100% completion rate.
Recruitment
The first three questions were designed to ensure that individual answering the survey met the recruiting criteria. All nine respondents replied to all three questions leading the investigators to believe they did indeed meet the recruiting criteria. Interestingly, the third question which asked respondents to identify their individual job titles was quite heterogeneous, demonstrating the wide variety of titles a nurse might have at the senior executive level. The results of the first three questions gave the PI confidence that the recruiting strategy had been successful and that the results would reflect high levels of confidence.
Question #3
Senior healthcare executives and leaders may be identified with many possible titles, even a combination of titles, to describe their position within a Health Authority. Some examples include: Chief Nursing Officer (CNO), VP Nursing Administration, Chief Nursing Information Officer (CNIO), Chief Executive Officer (CEO), Chief Information Officer (CIO), Chief Quality Officer, Chief Operating Officer (COO), Chief Financial Officer (CFO), President, Vice-President, Director, and Associate Director. What is your current title, or the title that best describes your current position or role within the Health Authority?
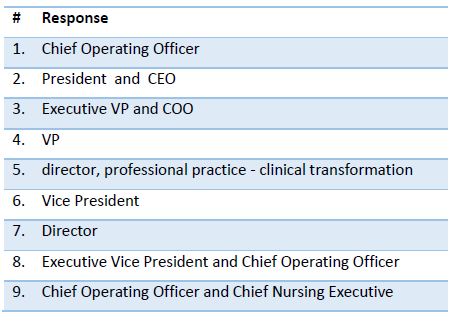
Figure 1- Declared Job Titles
Demographics
The demographics section of the survey questionnaire demonstrates our respondents are very experienced nurses, very well educated within traditional nursing programs, though often many years ago. Many are also well educated in graduate level business programs, come from a wide variety of clinical backgrounds, but demonstrate some significant differences when it comes to years of experience in their executive positions.
Question #4
Please tell us how many years’ experience you have in clinical nursing (in any practice setting)?
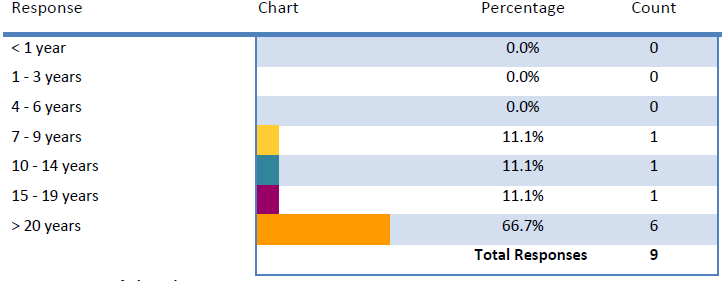
Figure 2- Years of Clinical Nursing Experience
Question #5
Please tell us how many total years’ experience you have in your current or similar position/role (in a healthcare executive/leadership role)?
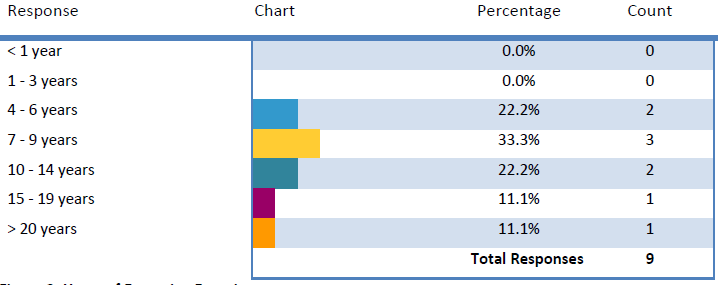
Figure 3- Years of Executive Experience
Question #6
What is your highest level of formal nursing education earned?
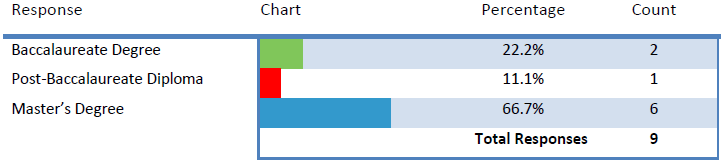
Figure 4- Highest Level of Nursing Education
Question #7
How long ago did you graduate from your most recent completed nursing program?

Figure 5- Years Since Graduation from Nursing Education
Question #8
Have you earned an advanced certificate/diploma/degree from a field outside nursing? Please select all that apply.
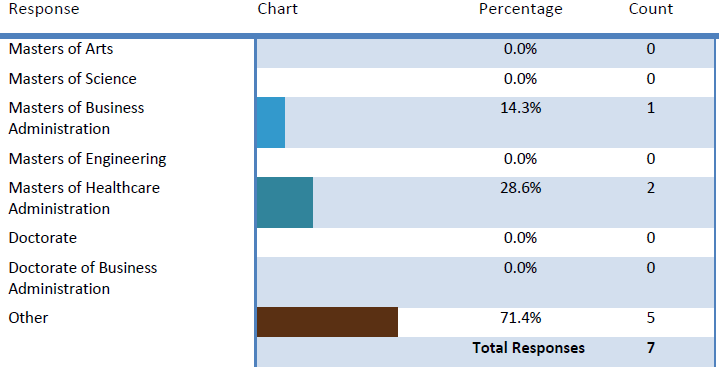
Figure 6- Education Outside Nursing
Question #9
What was your main area of clinical nursing practice before you accepted an executive/leadership position?
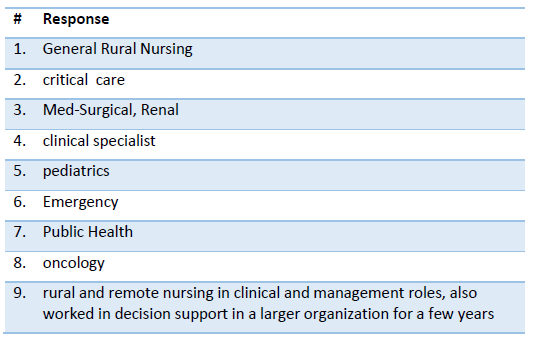
Figure 7- Clinical Nursing Background
Informatics Knowledge
Though only one respondent indicated formal education in informatics, all other respondents indicated at least some on-the-job training in informatics, and 8 of 9 even went so far as educating themselves on their own time on informatics subjects. This is a very positive and encouraging finding considering the importance of nursing involvement in the acquisition or upgrading of an EHI system, and is particularly encouraging considering the limited amount of free time an individual in an executive healthcare position would have available. Additionally, these respondents have indicated this work has real meaning for themselves, and the additional informatics knowledge each sought is purposeful.
Question #10
Do you have formal training in informatics? Informatics may be broadly defined using terms including (but not limited to) computer science, health informatics, and information sciences.
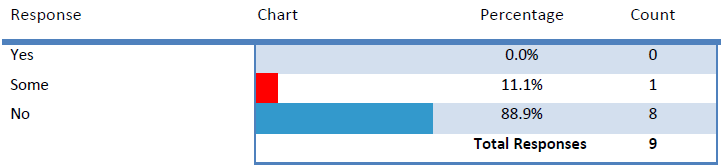
Figure 8- Formal Informatics Training
Question #12
Have you gained informal knowledge of informatics, health informatics or computer systems (such as electronic health records) on-the-job?
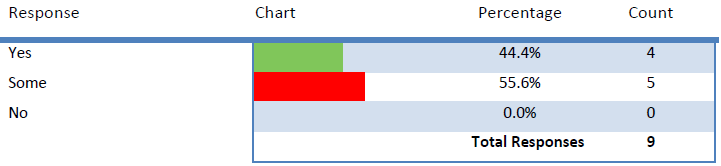
Figure 9- Informal Informatics Training (On-the-Job)
Question #13
Have you gained informal knowledge of informatics, health informatics or computer systems (such as electronic health records) through personal interest or study?
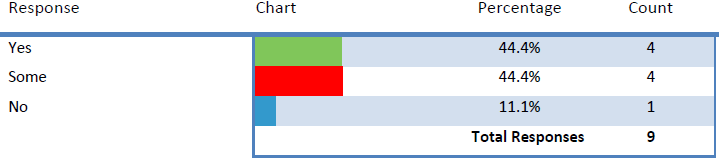
Figure 10- Informal Informatics Training (Personal Interest)
Informatics Experiences
The informatics experiences section of the survey questionnaire yielded some positive and encouraging findings. The majority (78%) of the senior healthcare executives in our study group have had experience in informatics project teams and most respondents indicated both non-trivial involvement and contributions. Many of our respondents have been invited to join IT project groups, and almost 40% were so interested, they asked to be included. All our nurse executives reported feeling welcomed by the IT staff, with a very few comments indicating some initial resistance that was later overcome as the teams began to work together as the project progressed. We also learned that nurse executives in our study were involved in some of the key financial decisions (78%) surrounding IT projects in their Health Authorities, and are open to input from a wide variety of sources when it came to improving their knowledge and understanding of informatics. We discovered that many of our respondents are involved in the evaluation stage of these projects, and many feel they have personally influenced a projects decision-making process in their respective Health Authorities.
Question #14
Are you currently, or have you been in the past, involved (to any degree) in any informatics (computer systems) acquisition or upgrading projects in your current (or previous) health authority (such as an electronic health records project)?

Figure 11- IT Project Experiences
Question #14(a)
If yes, how would you describe your degree of involvement on the project you had the most involvement in?
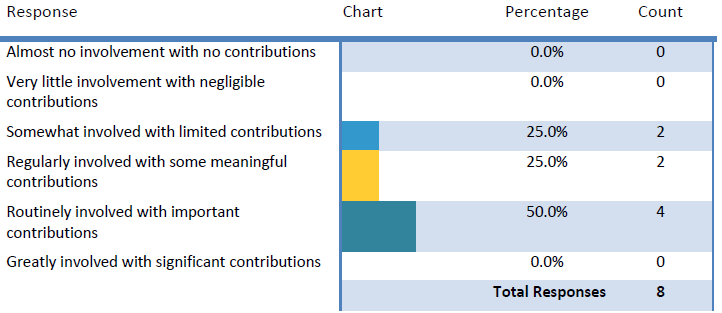
Figure 12- Degree of Involvement
Question #15
How was your participation solicited in any informatics (computer systems) acquisition or upgrading projects in your current (or previous) health authority (such as an electronic health records project)? Were you invited to participate in that project, assigned to that project, or did you ask to be involved? Please select all that apply.
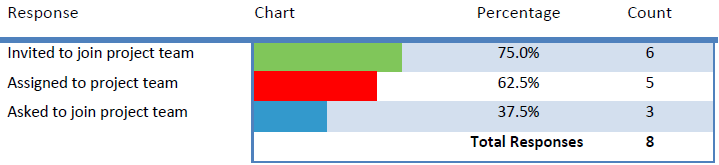
Figure 13- Invitation to Participate
Question #15(a)
If you were either assigned to, or asked to, join the project team (not invited), did you feel welcomed by the IT (Information Technology) group assigned to that project?
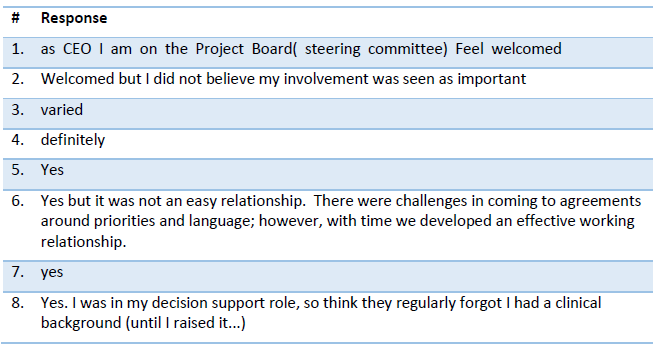
Figure 14- Feeling of Inclusion
Question #16
Have you been involved in any of the financial negotiations or decisions concerning the acquisition of an electronic healthcare information system?
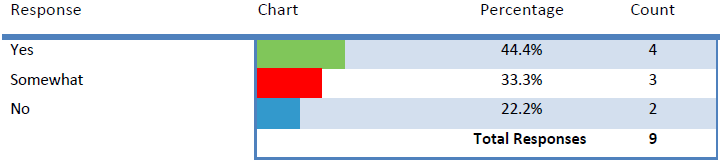
Figure 15- Involvement in Financial Decisions
Question #17
Who (or what) else do you rely on for additional information when a decision is required that involves an IT (Information Technology) component? Please check all that apply.
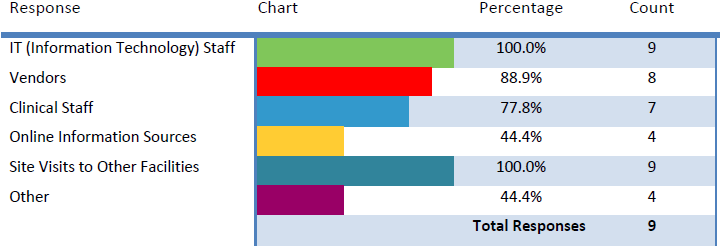
Figure 16- IT Project Assistance
Question #19
Have you ever been involved in the evaluation of a new, or upgraded electronic healthcare information system (such as an electronic health records system) after the system went live in your health authority?
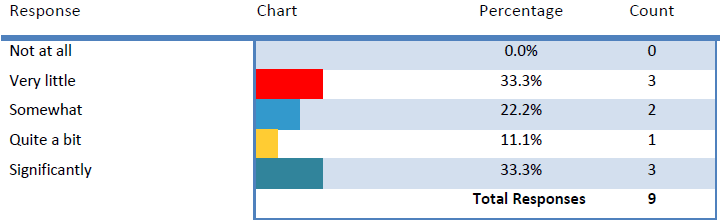
Figure 17- Project Evaluation Experience
Question #20
Do you feel as though you have personally influenced the procurement of electronic healthcare information systems (such as electronic health records) in your Health Authority?

Figure 18- Personal Influence
Informatics Attitudes
This section of the survey questionnaire succeeded in collecting many opinions and feelings from the nurse executive respondents in this study. Though most of the responses were subjective, they still offer interesting and important insights into how nurse leaders in British Columbia are thinking. We learned our participants feel very strongly that clinical users should guide informatics projects in their Health Authorities, but with significant support from their expert IT colleagues. Most respondents also felt that the IT staff do not believe clinical staff have enough knowledge to make informed decisions within EHI systems projects (suggesting opportunities for knowledge acquisition); regardless, these same executives also strongly believe that ‘Nursing’s Voice’ must be heard in EHI acquisition or upgrading projects.
Question #21
Regardless of your background, interest, or knowledge of information technologies, do you feel these types of decisions (such as the acquisition of a new electronic health record system) are best left to the IT (Information Technology) department?
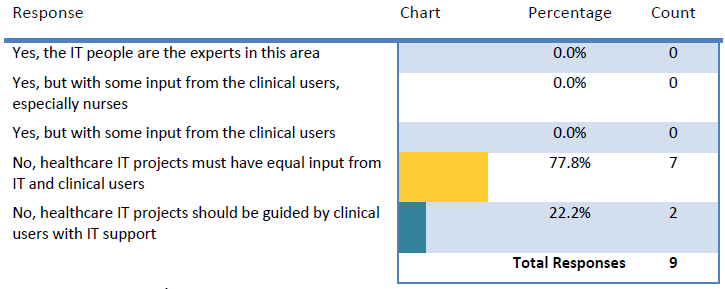
Figure 19- Decision-Making Opinion
Question #22
How much influence in healthcare IT (Information Technology) acquisition decisions do you believe is ideal for the following disciplines (percentages should add up to 100%)? Please check all that apply and enter % in text box next to each group.
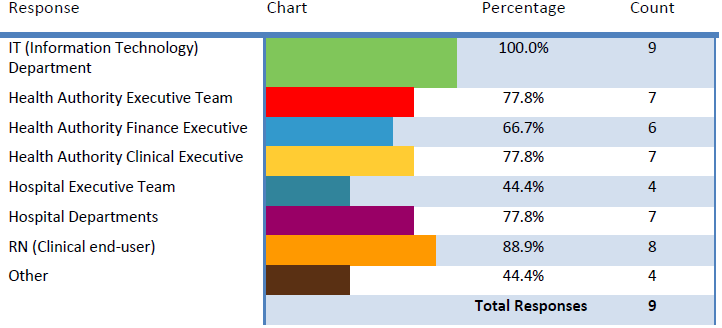
Figure 20- Departmental Influence
Question #23
In your opinion, do members of the IT (Information Technology) team feel clinical staff have the knowledge necessary to make informed decisions in the acquisition of new or upgraded electronic information systems?

Figure 21- IT Department Opinion
Question #24
Do you personally feel it is important for “Nursing’s voice” to be heard when IT (Information Technology) projects are planned? Should nurses be “invited to the table”?

Figure 22- Nursing’s Voice Opinion
Question #24(a)
It is very important that “Nursing’s voice” be heard when a Health Authority is planning the acquisition or upgrading of an electronic healthcare information system.

Figure 23- Nursing’s Voice Opinion (Ranking)
Study Limitations
The researcher acknowledges there are limitations to this study. First, it must be recognized that because this was a self-administered online questionnaire, the researchers have no way to fully verify the responses as entirely true. Secondly, the survey questionnaire design itself is lacking in some important areas that were discovered after responses were analyzed; a reflection of the inexperience of the PI. Third, the study sample size was small, and two potential respondents were away during the time the survey questionnaire was live; this leads to legitimate questions of external validity (generalizability) and the ability to extend the results obtained for the given sample to another population.
Discussion
Implications
Positive and encouraging are two words that first come to mind when reviewing the responses to the survey questionnaire. This author was pleasantly surprised with both the high response rate, and the content of the replies themselves. Clearly, our senior nursing executives in British Columbia felt they had something important to contribute to this discussion, as many not only answered the survey questions, but also added optional comments. Further, the responses indicate a real interest and participation in healthcare IT. Additionally, it would not be too difficult to assume the nurse executives in this study perceived this was work of some importance.
It was particularly encouraging to learn the majority of our respondents use personal time to increase their knowledge of health and nursing informatics. Equally impressive was learning the majority of our respondents also learned a great deal on-the-job. This speaks volumes about the willingness of the health informatics professionals and IT staff to include clinical staff in healthcare IT projects in a substantive way.
The nursing informatics experts recruited to participate in the pre-testing of the survey questionnaire were also all keen to be involved in this work, a clear and positive message that many of our top people in Canada feel this was a project of interest and value. All accepted their invitation to review, and their contributions were often substantial, as is obvious when viewing their detailed responses.
This research project was an attempt to expand our understanding of where nursing leadership fits into the process of acquiring a new or upgraded electronic healthcare information system. However, this study only examined nurses’ roles at the senior executive level in the province of British Columbia. Clearly there are opportunities to explore ‘Nursing’s Voice’ at other levels of clinical care, and in other provinces. It would be of real interest to also now consider these research questions at the level of middle management, and then perhaps the view from the bedside. It would be equally interesting to hear from the ‘other side’, the IT departments and health informatics professionals.
What might these finding mean to those in the nursing profession? These results are excellent news. The use of information technology in healthcare is only going to expand in the future, and nursing will need to embrace these changes. It would have been particularly concerning if the survey responses had indicated disinterest, or worse, hostility toward the adoption of EHI systems; even more concerning if coming from our nursing leadership. However, the responses did not indicate any such feelings, instead active involvement and interest, feelings it is hoped are passed down through the Health Authorities nursing staff.
What might these finding mean to health information science professionals? Again, excellent news. Individuals working on the non-clinical side of healthcare IT must be encouraged by these findings, to know that senior leadership in their Health Authority is keenly interested in the work they do and the contributions they make. Unfortunately, all too often non-clinical staff are made to feel somehow less important in the care team, largely because the work they do is “invisible” to patients and medical staff. These professionals provide key services in the form of information support which is relevant to the people carrying out the activities, the clinical staff. Perhaps knowing that our senior executive nurses share a strong interest in healthcare IT might be a small step in closing this divide.
What might these findings mean to educators in nursing and health information sciences? These findings may indicate a need for professional development courses, courses designed to be easily accessible to busy nursing executives. The survey questionnaire should have added a question concerning access to relevant health or nursing informatics education; this added layer of depth could have proved valuable, particularly to the co-supervisors on this project. Educators may also want to review current curricula in their baccalaureate and masters programs. This survey clearly showed that formal informatics training was not a part of our respondents’ education, though for a variety of well understandable reasons. It is also well known that schools of nursing incorporate very little informatics training into their curricula, at any level. However, our leaders of the future need this education now if they are to be prepared for their future roles. And this training can come from within nursing schools or from educators in other appropriate departments, such as health informatics. Regardless, advances in healthcare IT will not wait: curriculum changes need to be made sooner rather than later.
What are the implications for executives and leaders? It is hoped these results will increase awareness of the ever-growing important role IT plays in healthcare, and the increasingly important role clinical staff should play in healthcare IT projects as well. Future nurse executives would be well served if they understood now, the roles they may take on and the healthcare informatics training they will need in the future.
Conclusion
The purpose of this research was to develop a better understanding of senior nurse executives’ participation in the acquisition of a new or upgraded electronic healthcare information system; does nursing have a voice at this table? Based on these results it appears nursing does contribute at this level, and these results are very positive and encouraging. The philosophy and practice of involving the end-users, or the leaders of those end-users, in large information technology projects has grown in acceptance; grown to the point it is now seen as a vital component in optimal software systems design. It is heartening to see that, at least among our small group of respondents, this practice has seen significant adoption.
Bibliography
Academy of Canadian Executive Nurses. (2011). Leadership for health system transformation: What’s needed in Canada? Brief for the Canadian Nurses Association’s national expert commission on the health of our nation – The future of our health system. Retrieved from http://www.acen.ca/files/ 2012/06/ACEN-Leadership-for-Health-System-Transformation-October-2011.pdf
American Organization of Nurse Executives. (2009). AONE guiding principles: For the nurse executive to enhance clinical outcomes by leveraging technology. Retrieved from http:// www.aone.org/resources/ PDFs/AONE_GP_Leveraging_Technology.pdf
American Organization of Nurse Executives. (2010). AONE guiding principles: For defining the role of the nurse executive in technology acquisition and implementation. Retrieved from http://www.aone.org/resources/PDFs/AONE_GP_Technology_and_Acquisition_and_Implementation.pdf
American Organization of Nurse Executives. (2012). AONE guiding principles: For the chief nurse executive, chief information officer and industry partners to work together to leverage technology to enhance clinical outcomes. Retrieved from http://www.aone.org/resources/PDFs /AONE_GP_for_Nurse_ Exec_CIO.pdf
Beard, E. (2006). The CNO and “techies”: A dynamic duo. Nursing Management, 12, 53-60.
Bennett, C., Khangura, S., Brehaut, J., Graham, I., Moher, D., Potter, B., & Grimshaw, J. (2011). Reporting guidelines for survey research: An analysis of published guidance and reporting practices. PLOS Medicine, 8(8), 1-11.
Borycki, E, Frisch, N, McIntyre, M, & Kushniruk, A. (2011). Design of an innovative double degree graduate program in health informatics and nursing: Bridging nursing and health informatics competencies. European Journal for Biomedical Informatics, 7(2), 31–39.
Buntin, M, Burke, M, Hoaglin, M, & Blumenthal, D. (2011). The benefits of health information technology: A review of the recent literature shows predominantly positive results. Health Affairs, 30(3), 464-71.
Canada Health Infoway. (2013). Adoption. Retrieved from https://www.infoway-inforoute.ca/ index.php/progress-in-canada/benefits-realization/ adoption
Canadian Association of Schools of Nursing (CASN). (2012). Nursing informatics competencies: Entry-to-practice competencies for registered nurses. Retrieved from http:// www.casn.ca/en/
Canadian Nurses Association. (2006). Nursing information and knowledge management. Retrieved from http://cna-aiic.ca/en
Canadian Federation of Nurses Unions. (2011). The nursing workforce. Retrieved from http:// www.nursesunions.ca/sites/default/files/ 2012.backgrounder.nursing_workforce.e_0.pdf
Cipriano, P. (2012). The importance of knowledge-based technology. Nursing Administration Quarterly, 36(2), 136–146.
Coughlan, M., Cronin, P., & Ryan, F. (2009). Survey research: Process and limitations. International Journal of Therapy and Rehabilitation, 16(1), 9-15.
COACH. (2012). Health informatics professional core competencies. Retrieved from http:// coachorg.com/en/publications/resources/Core Competencies-New_Matrix_Nov_09.pdf
FluidSurveys. (2014). FluidSurveys. Retrieved from http://fluidsurveys.com/
Health Information Management and Systems Society. (2012). Certified professional in healthcare information and management systems (CPHIMPS) Certification. Retrieved from http://www.himss.org/content/files/ FAQ%20for%20CPHIMS.pdf
Healthcare Quarterly. (2010). Canada’s healthcare providers. Retrieved from www.longwoods. com/product/download/code/19504?
Hersh, W. (2009). Health and biomedical informatics: Opportunities and challenges for a twenty-first century profession and its education. IMIA Yearbook of Medical Informatics, 138-145.
InspireNet. (2014). InspireNet. Retrieved from http://www.inspirenet.ca/
Jackson, W., & Verberg, N. (2007). Methods: Doing Social Research. 4th ed. Toronto: Pearson.
Kasunic, M. (2005). Designing an effective survey. Pittsburgh: Carnegie Mellon University Press.
Kung, D. (2013). Object-oriented software engineering: An agile methodology. New York: McGraw-Hill.
Larman, C. (2005). Applying UML and patterns: An introduction to object-oriented analysis and design and iterative development. 3rd ed. Philadelphia: Prentice Hall.
LoBiondo-Wood, G., & Haber, J. (2010). Nursing research in Canada: Methods, critical appraisal, and utilization. 3rd ed. Toronto: Elsevier.
PricewaterhouseCoopers. (2013). The emerging benefits of electronic medical record use in community-based care. Retrieved from http://www. documentcloud.org/documents/690256-final-infoway-emr-benefits-english-summary.html
Procter, P, Hayward, R, Heyes, B, & Owen, A. (2013). Encouraging nurses to take the lead on the information agenda. Nursing Management, 19(9), 26-28.
Remus, S., & Kennedy, M. (2012). Innovation in transformative nursing leadership: Nursing informatics competencies and roles. Nursing Leadership, 25(4), 14-26.
The Guardian. (2014). Research and development for start-ups. Retrieved from http://www. theguardian.com/media-network/media-network-blog/2014/jul/07/innovation-r-and-d-startups-live-discussion
The Online Journal of Issues in Nursing. (2010). Informatics: Electronic personal health records: Nursing’s role. Retrieved from http://www.nursingworld.org/MainMenuCategories/ ThePracticeofProfessionalNursing/Health-IT/Electronic-Personal-Health-Records.html
Yale University School of Nursing. (2011). Sybil Palmer Bellos lecture. Retrieved from http:// nursing.yale.edu/sybil-palmer-bellos-lecture-0
Biographical Statements
Allen McLean
Allen MCLEAN (PhD(c), University of Saskatchewan; email: jam532@mail.usask.ca)
Allen is currently a PhD student in Computer Science at the University of Saskatchewan in the Computational Epidemiology and Public Health Informatics Lab. His research interests include the development of computer modeling and simulation software for addressing health systems challenges, chronic diseases and health inequities at the population level, as well as machine learning techniques applied to large health datasets. Allen previously attended the University of Victoria earning an MN and MSc (Health Information Science) in a unique dual degree program for Nursing Informatics professionals. Allen has over 20 years’ experience in healthcare as an ultrasound technologist, clinical educator, team leader and community health RN.
Noreen Frisch
Noreen FRISCH (Professor, University of Victoria; email: nfrisch@uvic.ca)
My academic career includes appointments at four post-secondary institutions in Canada and the US. Over the years, I have maintained two areas of interest: Commitment to the philosophy and ideals of holistic nursing practice & Development of nursing standardized terms and evaluation of how nurses use such terms to articulate and document their work. I’ve published in the area of holistic theory and practice and worked with colleagues for over a decade to develop standards of practice for holistic nursing care. I’ve also studied the concepts of nursing diagnoses, documentation of nursing outcomes and standardized nursing languages as needed by nurses who face the move to electronic health records and digital recording of nursing data. As a nurse certified in holistic nursing, I am committed to use of technologies in service of holistic practice. I am very interested in supporting nurses to conduct their work and in supporting our discipline to document nursing’s contributions to client care outcomes. My current work involves use of a web-based platform making full use of Web 2.0 and social media to connect nurses in a network that supports nursing health services research.
Abdul Roudsari
Abdul ROUDSARI (Professor, University of Victoria; email: abdul@uvic.ca)
Abdul Roudsari received his BSc, MSc, and PhD. from London University with his PhD research being undertaken at Kings College London. Before joining the University of Victoria he taught at a number of higher education institutions in the United Kingdom. He was Professor of Health Informatics and Director of the Centre for Health Informatics (CHI) at City University London. He has been a member of the Centre since 1989, having had a particular involvement in a range of research projects concerned with the provision of decision support systems to diabetic patients. He has led a major innovative EU-funded home telecare project. This project has enabled the Centre’s already large number of international collaborations to be extended to groups in Portugal and Estonia.
Science graphic by Freepik from Flaticon are licensed under CC BY 3.0.
Made with Logo Maker




Recent articles
- Index of volume 21 number 221 Jun 2026
- What does Canada’s new National Artificial Intelligence Strategy mean for healthcare?21 Jun 2026
- UN SDGs and Open Source Principles as Outcomes and Implementation Approach to Health Informatics21 Jun 2026
- Designing Compassionate Systems: Why Nursing Must Lead in the Age of AI21 Jun 2026
- Advancing Nursing Informatics Through the Integration of Genomics: Addressing Barriers and Capacity Building in Canadian Healthcare21 Jun 2026