
All Systems Go: The Voice of Nurse Practitioners Using Electronic Patient Records

By Amy Sczelecki RN, BSc, BScN, MN(c), Ashley White RN, BSc, BScN, MN(c)
& Christina Hurlock-Chorostecki NP, PhD
Introduction
Background and Significance
 Electronic patient record systems have become an integral component of the Canadian healthcare system, introduced to improve the delivery, coordination, and quality of patient care. This vital technology is a cost-effective order entry method for healthcare providers designed to decrease redundancy in the system, facilitate work flow, improve clinical decision making, and decrease medication errors (Yan, Gardner, & Baier, 2012). Electronic patient record systems have many advantages over traditional paper charting such as; the ability to access and organize information, monitor changes in patient outcomes, track required appointments and follow-up care, and improve communication of patient information among care providers, thus improving the quality and safety of patient care (Hoonakker, et al., 2013; Hoonakker, Caron, & Walker, 2010; McMullen et al., 2014). The electronic patient record system is able to notify prescribing providers of current medication use, allergies, potential drug interactions, health history, and other relevant patient data, reducing the occurrence of adverse medication errors (McMullen et al., 2014; Narcisse, Kippenbrock, Odell, & Buron, 2013). Despite the numerous advantages electronic patient record systems offer, many barriers and dissatisfaction exists, preventing healthcare providers from efficiently and effectively using this healthcare technology.
Electronic patient record systems have become an integral component of the Canadian healthcare system, introduced to improve the delivery, coordination, and quality of patient care. This vital technology is a cost-effective order entry method for healthcare providers designed to decrease redundancy in the system, facilitate work flow, improve clinical decision making, and decrease medication errors (Yan, Gardner, & Baier, 2012). Electronic patient record systems have many advantages over traditional paper charting such as; the ability to access and organize information, monitor changes in patient outcomes, track required appointments and follow-up care, and improve communication of patient information among care providers, thus improving the quality and safety of patient care (Hoonakker, et al., 2013; Hoonakker, Caron, & Walker, 2010; McMullen et al., 2014). The electronic patient record system is able to notify prescribing providers of current medication use, allergies, potential drug interactions, health history, and other relevant patient data, reducing the occurrence of adverse medication errors (McMullen et al., 2014; Narcisse, Kippenbrock, Odell, & Buron, 2013). Despite the numerous advantages electronic patient record systems offer, many barriers and dissatisfaction exists, preventing healthcare providers from efficiently and effectively using this healthcare technology.
Nurse practitioners (NPs) are autonomous prescribing providers (care providers with legal authority to prescribe diagnostic testing and medications) who play a pivotal role in the delivery of healthcare services and are in a unique position to act as agents of change, influencing important decisions pertaining to Canada’s healthcare system (Narcisse et al., 2013). Their direct care roles position them as leaders in the effective use of health technology to improve the quality and efficiency of healthcare services (McQuade-Jones, Murphy, Novak, & Sarnowski, 2014). Therefore, it is critical that we understand the barriers and facilitators NPs experience when using electronic patient record systems to advocate for system development that is advantageous for NPs to use. Electronic patient record systems can ease documentation when prescribing providers are given the time and opportunity to learn the system and tailor it to their needs. Once the prescribing provider is familiar with the basics of how the system works, they are likely to see the ways in which the system can save time and improve the quality of their documentation (Bosch, 2014). It is important that the system is designed to meet the needs of each individual care provider and that these individuals take advantage of the training offered and continue to seek out new learning opportunities long after the system is in place to ensure successful implementation and continued use (Bosch, 2014). It is imperative for electronic system designers and healthcare administrators to listen and respond in a positive manner to the suggestions and concerns of clinical users to ensure user satisfaction, appropriate technology adoption, and quality of care (Sittig, Krall, Kaalaas-Sittig, & Ash, 2005).
Problem
The electronic patient record system, referred to as HUGO (Healthcare Under Going Optimization), was implemented throughout hospitals in Southwestern Ontario in 2014. HUGO was designed with the traditional hierarchical approach to care in which the physician enters an order for other care providers to follow. Several aspects of the traditional approach of HUGO that make it valuable for physicians, pose challenges for NPs as autonomous prescribing providers. Key areas requiring improvement for NPs include the limitation of assigning a single “most responsible provider” (MRP), receiving important patient results into their ‘message center’ (an automated results reporting inbox), order designs that limit NPs from admitting and discharging patients, prescribing medications, ordering tests that are within NP scope of practice, and ordering tests through the use of medical directives. As the number of practicing NPs continues to grow and the NP scope of practice continues to expand, it is becoming increasingly important that NPs have a usable and reliable electronic system that easily integrates their role into the computerized patient record system.
Intended Improvement
All Systems Go is a quality improvement (QI) project designed to evaluate the barriers, facilitators, and learning needs of NPs in three Ontario academic hospitals when using the HUGO system. QI involves the use of structured methods and models to improve care for patients and their families, and to improve practice for healthcare staff (Health Quality Ontario, 2012). The project aims to gather the experiences, challenges, and satisfaction of NPs using the HUGO electronic patient record system and to gain an understanding of their learning needs in relation to the newly implemented system.
The Plan-Do-Study-Act (PDSA) cycle was the framework used to determine which components of the HUGO system pose the greatest challenge and outline key suggestions for implementing positive changes to improve NP-user satisfaction. A summary of key results will be shared with key leaders to advocate for realistic solutions to identified barriers and challenges.
Process
The PDSA cycle is a useful framework for developing, testing, and implementing change for improvement purposes in healthcare settings (NHS Institute for Innovation and Improvement, 2008). It is a powerful framework for structuring a QI project and is comprised of four main stages (Health Quality Ontario, 2012). Plan, is where objectives and predictions are identified and a plan is developed to implement and test the change. Do, involves developing potential interventions, carrying out the test or change on a small scale, and documenting problems or unexpected observations. Study, is where the data is analyzed and compared to one’s predictions. Reflections are made on what was learned. Act, is when modifications are made, and preparation for the next PDSA cycle is implemented (Institute for Healthcare Improvement (IHI), 2011).
Using PDSA cycles are important because they allow modifications to be refined. Many problems that are encountered in the previous PDSA cycle can be resolved prior to the next PDSA cycle, making the implemented change more successful and sustainable (IHI, 2015). Furthermore, it is suggested that by running multiple tests, resistance to change is often alleviated and buy-in from stakeholders is more likely to be achieved (IHI, 2015).
Plan
The planning stage involved organizing the method for identifying objectives and key issues, engaging with key stakeholders, collecting and analyzing data, and setting measurable goals for meeting the objectives. We created a fishbone diagram (a cause and effect diagram), as a method of brainstorming several possible causes responsible for the challenges or issues NPs experience (see Figure 1). Creating a fishbone diagram allowed the QI team to address all possible causes of a problem, rather than focusing on only one possible cause (Health Quality Ontario, 2012). Engagement with key stakeholders, consisting of acting members of the E-Practice Sub-Committee, NP-users, and a lead Physician Informatics Specialist for the HUGO system, allowed us to identify relevant and pertinent barriers to NP usability within the HUGO system. Focus was given to barriers that are amendable to change rather than legislative or policy issues. A plan for disseminating the results was also initiated in order to ensure the voices of NPs are heard and the results of the QI project are shared with key stakeholders and participants to address system issues and promote positive change.
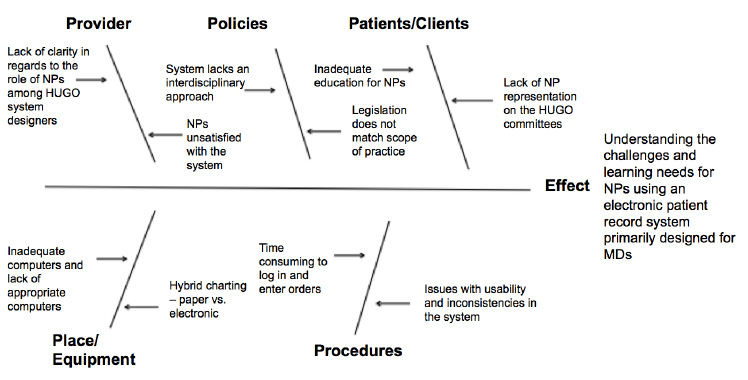
Figure 1: Fishbone diagram created as a method of brainstorming in which several possible causes responsible for the challenges or issues NPs experience when using the electronic patient record system were identified
Do
In the Do stage, a non-experimental, cross-sectional survey design was conducted using a self-report questionnaire to evaluate the barriers, facilitators, and learning needs of the NPs using the HUGO system. NPs employed at the hospitals were asked to complete a short web-based survey consisting of 15 questions, which aimed to identify specific functionalities NP-users felt needed to be modified or improved to better suit their needs as prescribing providers. Survey questions varied in format consisting of close-ended, open-ended, and multiple-choice questions to extract the most modifiable barriers. Specifically, in order to collect important information about the barriers hindering the entering of patient care orders and the usability of the HUGO system, participants were asked to select their top five issues from a list of identified concerns and were invited to provide their own issue not included in the list as a free text comment. Participants were encouraged to be as specific as possible when responding to the survey questions to allow for a detailed description of the necessary system modifications when presenting the results.
The web-based survey was e-mailed to all NPs currently using the HUGO system (n=67). Participants were given a brief description of the QI project and were provided with a hyperlink directing them to the survey. A web-based survey was chosen because they often increase participant motivation to respond due to interactive features and the ability to provide detailed information about their responses (Polit & Beck, 2012). Furthermore, they are advantageous as they result in data directly available for analysis. To further increase participation, reminder e-mails were sent to all potential participants one week and 48 hours prior to the closing of the survey. The overall response rate for survey completion was 45%.
Study
In the study stage, survey results were collected and analyzed. Amendable changes to improve ease of use and efficiency for NPs were identified and results were summarized to allow for reflection on the information collected. Pareto diagrams were created for the two questions that asked participants to select their top five issues with entering patient orders, and using and viewing patient charts. Pareto diagrams are based on the 80/20 rule stating that 80% of the problem results from 20% of the causes (IHI, 2015). They help to determine the root cause of the issue and highlight the problems to prioritize. The Pareto analysis allowed us to focus our efforts on issues that offer the greatest potential for improvement. Learning needs were evaluated to determine appropriate training opportunities for implementation to improve continued usability and NP-user satisfaction.
Results
NP respondents were employed in either inpatient (30%) or outpatient (23%) practice settings with the majority of NPs practicing in both inpatient and outpatient areas (47%). More than half of NPs revealed entering 10 or more inpatient orders into the HUGO system daily, with 43% entering 20 or more inpatient orders each day. In contrast, only 33% enter 10 or more outpatient orders each day. To collect information about NP use of specific functionalities of HUGO, participants were asked to select the top five ways that they use the HUGO system as part of their workday. NPs primarily use the HUGO system for viewing results (100%), entering medications (90%), viewing past clinical notes (80%), and entering lab (73%) and diagnostic test orders (70%). Only 17% of NPs use the system to enter patient notes and 55% are either not aware of the Advanced Clinical Note module (ACN) as a method of typing patient notes, or lack the necessary education to use this function.
According to the Pareto diagram (see Figure 2), NPs reported that 80% of their problems when entering patient care orders stem from the following:
(1) There are many unnecessary steps and questions asked when entering orders,
(2) Having to flip back and forth between computer screens to view patients’ results, medications, and orders was confusing and time consuming
(3) At times, the computers would freeze and the system network was often slow,
(4) NPs often felt that they were expected to remedy incorrect orders entered by another prescribing provider, and
(5) The need to refer to both paper and electronic charting was confusing often resulting in iatrogenesis.
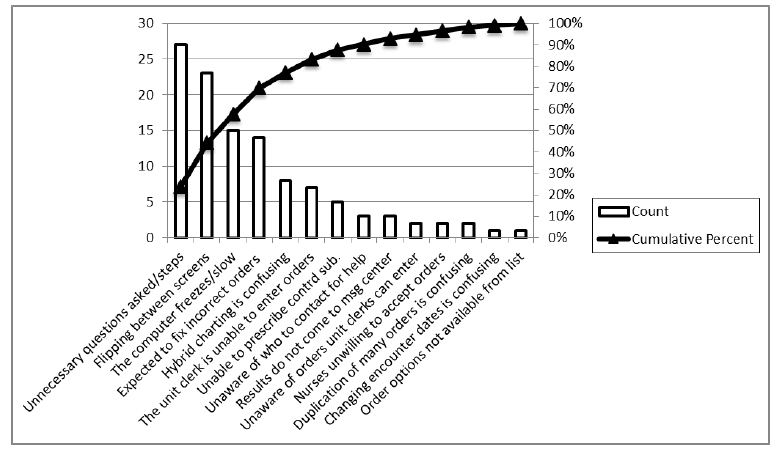
Figure 2: Pareto diagram displaying nurse practitioners’ key issues occurring when entering patient care orders into the electronic patient record system.
NPs reported similar findings when using and viewing electronic charting (see Figure 3). Key challenges identified were:
(1) The use of both paper and electronic charting was confusing and time consuming,
(2) The system lacks appropriate charting templates or key order sets,
(3) Results do not come to the message center as NPs are not listed as the MRP, and
(4) At times, the computers would freeze and the system network was often slow,
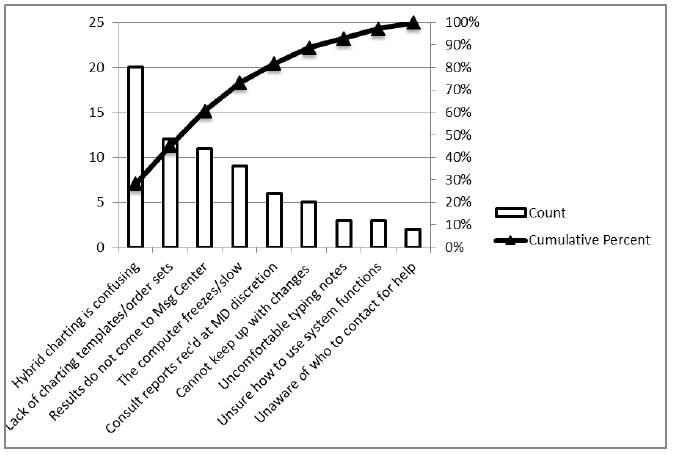
Figure 3: Pareto diagram displaying nurse practitioners’ key issues occurring when using and viewing electronic patient records.
Answers to questions pertaining to the quality of the electronic patient record system or available electronic equipment revealed that the majority of NPs are not satisfied with the computers they are using, stating they are not adequately meeting their practice needs. Common complaints identified were the small size of the available computer screens and the speed in which the electronic patient record system performs (see Figure 4).
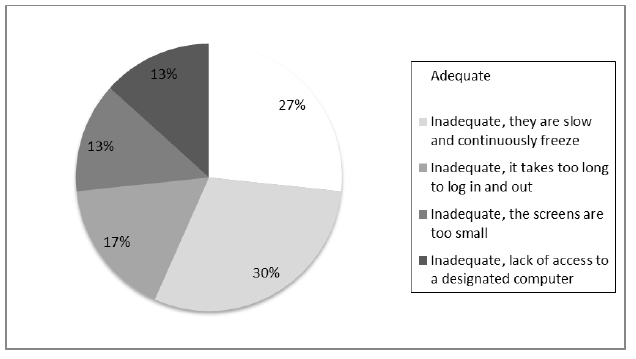
Figure 4: Main issues associated with the computers used for electronic order entry identified by nurse practitioners.
To assess the adequacy of NP education received during the implementation of HUGO, NPs rated their education from inadequate to very helpful. Sixty-nine percent reported that the HUGO training they received was inadequate stating it was not relevant to their practice needs or clinical setting. Specifically, NPs practicing in outpatient settings commented that education was geared towards those working in an inpatient setting. Moreover, the majority of NP participants expressed an equal need for education sessions related to order entry, ACN, Juniper (off-site access program), building ‘order favourites’, and tips to speed up the ordering process. Educational strategies of interest to participants included, NP specific training sessions, one-on-one training, drop-in sessions, and telephone support. Overall, it was determined that 79% of participants are somewhat satisfied with the current HUGO system and feel the system offers many key advantages in comparison to the previous method of paper charting (see Figure 5).

Figure 5: Advantages of using the electronic patient record system over traditional paper charting methods identified by nurse practitioners.
Act
In the act stage the change ideas were defined and refined based on the survey data. In conjunction with our key stakeholder and the results depicted from the Pareto diagrams, we were able to address some of the key issues causing end-user dissatisfaction among NPs. Results and suggested improvements were submitted to the region’s E-Practice Sub-Committee, Medical Affairs, and Nursing Professional Practice. Survey findings and an immediate education solution were distributed to all employed NPs. The strategies to advocate for improved NP HUGO usability and satisfaction were provided. Lastly, a poster was created summarizing the QI project for dissemination and presentation of results at the local and provincial level.
Discussion
There are many barriers and learning needs that coincide with the implementation of an electronic patient record system that can hinder user satisfaction and efficiency of the system. Top issues identified that affect prescribing providers include: Many unnecessary steps and questions asked, flipping back and forth between computer screens is time consuming, the computers freeze and the system network is slow, and the use of both paper and electronic charting is confusing. Additionally, NP specific issues identified from the survey result from the incomplete integration of the NP role as an equal member of the healthcare team. These issues include, the expectation that NPs will fix orders entered by another prescribing provider, a lack of charting templates and order care sets available for NPs to use, and a failure to recognize the NP as the MRP preventing patient care results from being sent to their message center inbox.
While it is recognized that entering patient orders is time consuming due to the many unnecessary questions asked and number of steps involved in the ordering process coupled with the cumbersome task of having to flip back and forth between computer screens, there are limited solutions that can be implemented as this problem is largely attributed to how the system was designed. However, when addressing these aforementioned issues with our key stakeholder, it was highly recommended that NPs provide the clinical informatics department with detailed information about the issue in the chance that change can be implemented. Furthermore, frustration from flipping through computer screens to view patient care information, may be reduced if prescribing providers open two separate patient care records simultaneously on their computer or utilize two computer monitors for ease of visibility.
It is evident that many of the NPs are frustrated with the speed of the system. The majority of participants identified various aspects of the system as being time consuming or slow to operate. Currently, the system is set up with a local data center and server that is unable to adequately manage the system’s capacity. To address this issue and increase the speed and storage capabilities of the HUGO system, the hospitals are in the process of moving the physical data center and servers to a remotely hosted secure location in Toronto with built-in double redundancy. In other words, there will be two data centers running in tandem, physically separated in case of catastrophic failure at one site. The remote host will be responsible for ensuring that system needs are met and upheld on a continual basis.
Another common frustration expressed by participants throughout the survey is the use of hybrid (electronic and paper) patient charting. During the transition to electronic patient records, many aspects of patient care have been duplicated, causing confusion and increasing the possibility for error. For example, one participant stated that electronic consults “go nowhere and you are still required to call the team” once they are entered into the system. One recommendation is to revise the current consult process. If initiated, the system can be designed to send an electronic consult to the corresponding team’s message center. For example, when cardiology is consulted, each member of the cardiology service will receive an alert through the message center pool. The provider that marks the alert as complete is then responsible for the consult and the alert is removed from the message center pool. To encourage the use of electronic consults and reduce discrepancies with suggested orders, the current consult process will be presented to the E-Practice Sub-Committee as an agenda item request for modification or change.
Due to financial constraints, the electronic patient record system is being implemented in stages. Hospital administration felt implementing HUGO, or computerized order entry, should receive priority over other electronic components such as electronic clinical documentation, referred to as Clindoc. Clindoc will allow care providers to complete all patient charting or documentation electronically, removing the use of paper. For example, patients’ vital signs are currently recorded on paper in bedside charts and allied health progress notes are located in paper charts at the nursing station, while admission, discharge, and summary notes are generally written electronically or dictated for entry into the electronic system. NPs describe this system as confusing and error provoking because it is difficult to locate all relevant aspects of patient information. Unfortunately, until further funding is received, care providers will be required to utilize both electronic and paper charts to gather all aspects of patient care.
When collecting information about issues related to entering patient orders into the HUGO system, many of the NPs expressed frustration with being expected to fix incorrect orders entered by another care provider. Although this is a valid concern, it is largely a communication or workflow related barrier to using the electronic system. A change in culture regarding the NP as a valued healthcare provider is needed. NPs must ensure they are advocating for their role and encouraging physicians to enter their own patient orders when possible. They must also inform the nursing staff that they should call the prescribing provider who initially entered the order for modification or discontinuation. Furthermore, when using and viewing the electronic patient record, NPs expressed concern regarding the limited availability of appropriate charting templates and order care sets. NPs need to engage with system development to correct this. Unfortunately, this was not done proactively despite recommendations during system creation. NPs must step forward and become champions in their role. Alternately, providers can create custom order sets and charting templates to meet their needs. To ensure NPs take advantage of this key system function, this learning need should be incorporated into future HUGO education training sessions.
In terms of consult results not coming to the NPs’ message center, this is not an issue that can be changed in the system; however, it is a shortcoming of the traditional approach to patient care where the physician enters the order and non-physician providers follow them. NPs must advocate for their needs and develop trusting partnerships with their physician colleagues encouraging and reminding the physicians to include them in receiving patients’ results.
QI initiatives are typically referred to as a process rather than an outcome (Gold et al., 2014). Careful planning and continuous discussion with key stakeholders is necessary to ensure the ongoing success of system improvements. PDSA cycles require the continuous evaluation of the issue and it is recognized that it will take time to ensure improved and ongoing NP-user satisfaction and efficiency with the electronic system.
Action: A Plan for All Systems Go
Through completion of the web-based survey, valuable insight was gained regarding the challenges and barriers NPs face when using the HUGO system. Areas for improvement to increase NP usability and satisfaction have been identified. The following actions will be taken.
Engaging NPs
Project findings have been shared with NPs, ensuring that their voices have been heard. Along with the findings, new knowledge was provided to the NPs regarding the use of the “4 help” button, a documented learning need. The use of this button will allow a quick, clear, and concise reporting of system challenges that can be addressed.
Engaging senior nursing leadership
An executive summary with specific recommendations was sent to hospital senior leadership and program directors regarding the importance of supporting time for NPs to attend HUGO related education. Prescribing provider education at the implementation of HUGO did not address NP specific nuances with ordering medications, ordering diagnostic tests, medication reconciliation, patient discharge, writing prescriptions, or entering problems and diagnoses. This must occur if we hope to sustain this vital electronic record system. As well, Advanced Clinical Notes (ACN) education has not been provided to all NPs. Time is needed to receive the appropriate education to use this electronic functionality. Another recommendation includes negotiating and supporting the creation of HUGO related processes that provide NPs with timely notification of patient results (such as within the “message centre”). The HUGO system is built to accommodate the traditional approach to healthcare, one doctor for each patient, which seldom exists today. This approach limits the work of the NP when they are not informed of laboratory or consultation results, causing delays to patient care, potential for medical error, an increase in hospital length of stay, and increased patient dissatisfaction.
Partnering with Medical Affairs
Medical Affairs is responsible for prescribing provider training; therefore, it is critical that they are involved in overcoming many of the barriers and learning needs highlighted in this QI project. It is recommended that medical affairs assist with the development and delivery of NP specific education for new and established NPs employed in hospitals using the HUGO system. This education is similar to the physician and medical resident “provider” education but would include nuances such as diagnostic imaging restrictions, prescribing restrictions, and medication reconciliation challenges.
It is vital that Medical Affairs communicates with physicians and medical residents about the importance of NPs as valued members of the healthcare team and as such should be included in patient related communication within and between program teams. All employed NPs have access to the “message centre” thus it can be easily included when other providers are documenting patient progress. Physician specialists need to be encouraged to include the NP on consultation reports, especially when the consult request is from the NP. Physicians should also be informed of the recent change to the Schedule of Benefits for Physician Services (May 2015) that supports referrals to specialists by NPs (Ministry of Finance, 2015; Ministry of Health, 2015). Lastly, Medical Affairs must work in collaboration with the Nursing Professional Practice Leaders at the region’s academic hospitals to design and implement a forward approach to changing the NP to MRP to meet the needs of patients (Ontario Hospital Association, 2012).
Education plans for NPs
Results revealed the need for improved NP specific education including computerized order entry training, ACN, and Juniper education sessions. The clinical informatics department has offered to facilitate an order entry refresher session using both a structured and unstructured format to address the variety of concerns NPs experience when using electronic patient records. During this education session, NPs will receive assistance related to their clinical needs in addition to receiving the mandatory training that is required to effectively and efficiently use ACN and Juniper.
To ensure NP attendance, education sessions will be approximately one hour in length and will be held at a time that is most convenient for NPs. Furthermore, a dinner and education in-service regarding the HUGO system will be provided for NPs at the region’s network meeting in the near future to discuss system improvements and NP learning needs.
Collaborating with clinical informatics
In order to alleviate identified barriers and learning needs with the electronic system, it is important for NPs to remain engaged with the clinical informatics department including information technology (IT) to ensure changes occur. In conjunction with this department, three modifiable barriers have been selected for submission as agenda items to the region’s E-Practice Sub-Committee to help improve NP-user satisfaction of the current electronic system. The first recommendation includes a revision of the current consultation method, developing a fully electronic consultative process using a message center pool. The initiation of this system function will allow a prescribing provider to send an electronic consult request to the corresponding team’s Message Center. Modifying the consult process to remove the paper component can reduce confusion associated with hybrid charting, prevent errors in which consults are missed, and reduce discrepancies associated with ‘suggested’ orders.
The second recommendation is the implementation of the message center to all providers, nursing, allied health, and secretaries with full functionality to allow for effective communication between team members and the ability to set reminders for clinical events or follow-up tasks.
Lastly, we recommend the implementation of Tap In/Tap Out access for all providers across the hospitals in order to facilitate faster logins and a decreased disruption of workflow. Detailed descriptions of the suggested changes will be included in the templates to increase the likelihood of the proposed modifications being implemented. Continued involvement and discussion with the E-Practice Sub-Committee will commence to advocate for the needs of NPs to ensure their voices are heard.
Limitations
First, we did not formally validate the questionnaire. However, prior to distributing the survey to potential participants, four NPs in various practice settings and the HUGO Physician Informatics Specialist reviewed or trialed the survey in order to provide feedback regarding the clarity and relevance of each survey question. As a key stakeholder, the Informatics Specialist validated the suspected barriers and facilitators of NPs experience with the HUGO system and provided information on which components of the system are eligible for change.
Second, the survey was administered electronically, requiring access to a computer and the perceived ability to complete an online questionnaire for those who are not familiar with the process. To avoid the risk of having the e-mail with the embedded hyperlink blocked by Internet security filters, the survey was sent from a hospital e-mail address. A third limitation is the use of self-report data to yield results. Although self-report measures are the most efficient for gathering information about what participants think, feel, or believe, they are liable to several response biases and contextual influences (Polit & Beck, 2012). Free text space was included to minimize bias, encouraging participants to express themselves freely and to expand on their own issues.
Furthermore, having NPs anonymously complete the study questionnaire on their own time aids in decreasing the effects of some of these influences and biases by ensuring confidentiality. Lastly, due to the complexity of the electronic patient record system, it is difficult for the informatics team to troubleshoot issues such as slowness and frozen screens. In order to investigate the cause of these issues, providers must document which screens were open and the time of occurrence. Since the survey was sent to all eligible NPs using the HUGO system, it is not possible to collect such detailed information. NPs will be encouraged to document these issues in the future and report each incident to the HUGO help desk for further investigation.
Conclusion
Research suggests that electronic patient record systems can improve patient outcomes, reduce clinical errors, and serve as a cost-saving alternative to traditional paper charting methods (Thurston, 2014). Electronic patient record systems, specifically computerized provider order entry, have been proven to increase efficiency and accuracy of healthcare services (Sittig et al., 2005). The implementation and usability of electronic patient record systems have stumbled due to lack of attention regarding end-user needs resulting in user dissatisfaction (Hoonakker et al., 2013). Understanding NP challenges and learning needs in relation to the electronic patient record system is critical for developing strategies to effectively improve the usability of the system and, in turn, improve patient care outcomes. The ‘All Systems Go’ QI project was designed to gather insight and understanding of the barriers and facilitators NPs face when using the electronic patient record system. The web-based survey yielded valuable information to address the lack of attention given to NP-user needs. As a result, three key system modifications were proposed and several educational opportunities were developed to address identified learning needs.
References
Bosch, J. (2014). Electronic medical records: My journey. The Journal for Nurse Practitioners, 10, 627-629. doi:10.1016/j.nurpra.2014.05.013
Gold, J., Reyes-Gastelum, D., Turner, J., & Davies, H. D. (2014). A quality improvement study using fishbone analysis and an electronic medical records intervention to improve care for children with asthma. American Journal of Medical Quality, 29, 70-77. doi:10.1177/106286061348171
Health Quality Ontario. (2012). Quality improvement guide. Retrieved from http://www.hqontario.ca/portals/0/Documents/qi/qi-quality-improve-guide-2012-en.pdf
Hoonakker, P. L., Carayon, P., Brown, R. L., Cartmill, R. S., Wetterneck, T. B., & Walker, J. M. (2013). Changes in end-user satisfaction with computerized provider order entry over time among nurses and providers in intensive care units. Journal of the American Medical Informatics Association, 20, 252-259. doi:10.1136/amiajnl-2012-001114
Hoonakker, P. L., Carayon, P., & Walker, J. M. (2010). Measurement of CPOE end-user satisfaction among ICU physicians and nurses. Applied Clinical Informatics, 1, 268-285. doi:10.4338/ACI-2010-03-RA-0020
Institute for Healthcare Improvement. (2015). Science of improvement: Testing changes. Retrieved from http://www.ihi.org/resources/Pages/HowtoImprove/ScienceofImprovementTestingChanges.aspx
McMullen, P. C., Howie, W. O., Philipsen, N., Bryant, V. C., Setlow, P. D., Calhoun, M., & Green, Z. D. (2014). Electronic medical records and electronic health records: Overview for nurse practitioners. The Journal for Nurse Practitioners, 10, 660-665. doi:10.1016/j.nurpra.2014.07.013
McQuade-Jones, B., Murphy, J., Novak, T., & Sarnowski, L. (2014). Nurse practitioners and meaningful use: Transforming health care. The Journal for Nurse Practitioners, 10, 763-768. doi:10.1016/j.nurpra.2014.08.004
Ministry of Finance Ontario (2015). Ontario Budget. Chapter 1: Providing faster access to the right care. ?Retrieved from http://www.fin.gov.on.ca/en/budget/ontariobudgets/2015/ch1f.html
Ministry of Health (2015). INFOBulletin #10047: Nurse practitioner referrals to physicians. May 8, 2015. ?Retrieved from http://www.health.gov.on.ca/en/pro/programs/ohip/bulletins/10000/bul10047.pdf
Narcisse, M., Kippenbrock, T. A., Odell, E., & Buron, B. (2013). Advance practice nurses’ meaningful use of electronic health records. Applied Nursing Research, 26, 127-132. doi:10.1016/j.apnr.2013.02.003
NHS Institute for Innovation and Improvement. (2008). Plan, do, study, act (PDSA). Retrieved from http://www.institute.nhs.uk/quality_and_service_improvement_tools/quality_and_service_improvement_tools/plan_do_study_act.html
Ontario Hospital Association (2012). Enabling nurse practitioners to admit and discharge: A guide for hospitals. Retrieved from https://www.oha.com/CurrentIssues/keyinitiatives/PhysicianandProfessionalIssues/Physicians/Resources/Documents/Final%20-%20NP%20Guide.pdf
Polit, D. F., & Beck, C. T. (2012). Nursing research: Generating and assessing evidence for nursing practice (9th ed.). Philadelphia, PA: Lippincott Williams and Wilkins.
Sittig, D. F., Krall, M., Kaalaas-Sittig, J., & Ash, J. S. (2005). Emotional aspects of computer-based provider order entry: A qualitative study. Journal of the American Medical Informatics Association, 12, 561-567. doi:10.1197/jamia.M1711
Thurston, J. (2014). Meaningful use of electronic health records. The Journal or Nurse Practitioners, 10, 510-513. doi:10.1016/j.nurpra.2014.05.012
Yan, H., Gardner, R., & Baier, R. (2012). Beyond the focus group: Understanding physicians’ barriers to electronic medical records. The Joint Commission Journal on Quality and Patient Safety, 38, 184-191. Retrieved from www.ncbi.nlm.nih.gov/pubmed/22533131
GRAPHIC
Person, Hand Drawn,Tool,Medical Tool, Stylish, Medicine, Watch graphics by Freepik from Flaticon are licensed under CC BY 3.0. Made with Logo Maker
Author Information
Amy Sczelecki RN, BSc, BScN, MN(c)
Western University, London Ontario asczele@uwo.ca
Amy Sczelecki is a registered nurse working in an acute care surgical setting at University Hospital in London Ontario. Amy is currently pursuing her Masters at the University of Western Ontario and is in her final year of the Primary Healthcare Nurse Practitioner Program.
Ashley White RN, BSc, BScN, MN(c)
Western University, London Ontario awhite47@uwo.ca
Ashley White is a registered nurse working in an acute care surgical setting at Victoria Hospital in London Ontario. Ashley is currently pursuing her Masters of Nursing at the University of Western Ontario and is in her final year of the Primary Healthcare Nurse Practitioner Program.
Christina Hurlock-Chorostecki NP, PhD
London Health Sciences Center, Victoria Hospital Tina.HurlockChorostecki@lhsc.on.ca
Christina Hurlock-Chorostecki is a Professor at the Labatt Family School of Nursing, Western University in London Ontario. She works in her Adult Nurse Practitioner role at the London Health Sciences Centre in London Ontario and represents NP interests within HUGO.

OUR SPONSORS

Visit the Nursing Informatics Learning Center for resources, courses, news, and other informatics related content.




Recent articles
- Index of volume 21 number 221 Jun 2026
- What does Canada’s new National Artificial Intelligence Strategy mean for healthcare?21 Jun 2026
- UN SDGs and Open Source Principles as Outcomes and Implementation Approach to Health Informatics21 Jun 2026
- Designing Compassionate Systems: Why Nursing Must Lead in the Age of AI21 Jun 2026
- Advancing Nursing Informatics Through the Integration of Genomics: Addressing Barriers and Capacity Building in Canadian Healthcare21 Jun 2026