
Enhancing Patient Safety by Mitigating Nursing Medication Administration Workarounds

by Heather Poland, RN MHA
Clinical Informatics Lead, BC Children’s & Women’s Hospital
Agnes Black, RN MPH
Director, Health Services & Clinical Research, Providence Health Care
Isabel Diogo, RN MSN
Practice Consultant, Medication Safety and Management, Providence Health Care
Citation: Poland, H., Black, A. & Diogo, I. (2023). Enhancing Patient Safety by Mitigating Nursing Medication Administration Workarounds. Canadian Journal of Nursing Informatics, 18(1). https://cjni.net/journal/?p=10862

Abstract
Closed Loop Medication Management [CLMM] and Barcode Medication Administration [BCMA] workflows are the gold standard for safe medication administration. However, workarounds continue to plague BCMA success, and globally up to 68% of medication administrations include a workaround. In February 2022, a hospital in western Canada had the opportunity to conduct a Quality Improvement (QI) initiative: the CLMM Nursing Workaround Mitigation Strategy, with the roll-out of the new electronic health record (EHR).
The purpose of the project was to determine whether a pre-emptive CLMM Workaround Information Session would enhance nurses’ understanding of workarounds and influence unit culture and attitudes towards leadership in a way that decreased the number of BCMA workarounds, thus improving patient safety. The effectiveness of the information session was measured via surveys and interviews.
Results showed that the information session improved nurses’ knowledge about CLMM, decreased the perception of workarounds as inherently “bad”, and increased direct care nurses’ feelings of motivation and empowerment to give feedback to leadership. Two months later this increased knowledge and motivation were still present. Those who participated in the information session also indicated a greater willingness to provide feedback to their leadership team regarding issues with CLMM. Similarly, nurses who participated in the interviews stated they had increased capacity to openly discuss workarounds with co-workers. While it was beyond the scope of this project to assess patient safety improvements following the information sessions, improved practice of CLMM and BCMA are clearly linked to improved patient safety.
Disclosure
This project was determined to be QI, and therefore no ethics review was required.
Introduction
Over the last 30 years, technology has played an increasingly important role in healthcare. Multi-million-dollar subsectors of health information technology [HIT] have been incorporated into health systems and subsequent Clinical Informatics departments have emerged to develop, implement, analyze, and optimize the intersection of medicine and information systems with the goal of improving the health and wellbeing of patients.
Closed Loop Medication Management [CLMM] is HIT in action, utilizing various individual HIT innovations in one end-to-end system with the goals of decreasing adverse medication events. Barcode Medication Administration [BCMA] represents a major change to the nursing portion of the medication administration workflow. Instead of relying on nurse vigilance to avoid medication errors, a barcode scanner is used to verify some of the medication “checks”- the correct patient, correct medication, correct dose, correct formulation, and correct time (Burkoski et al. 2019). This technology has become widespread and is hailed as a “simple” evidence-based way to reduce medication errors (Truit et al. 2016). However, various studies suggested a disconnect between the HIT developers and nurse implementers, with inadequate communication between HIT developers, Professional Practice Offices, and direct care nurses. Instead of following recommended workflows, nurses create and use workarounds, defined as “informal and/or temporary behaviours or actions that ‘fix’ perceived workflow hindrances to meet a goal or to achieve it more readily” (Debono et al, 2013, p. 1). Further investigation shows that BCMA workarounds can lead to a significant increase in medication errors, sometimes more than were seen with paper-based systems (Truitt et al., 2016; van der Veen et al., 2017).
As one urban hospital in western Canada prepared to roll out a new electronic health record (EHR) – including CLMM and BCMA workflows – there were concerns about workarounds and subsequent patient harm. A QI project to test a CLMM nursing workaround mitigation strategy was initiated, with the goal of improving nurses’ understanding of workarounds, reducing the incidence of workarounds, and increasing nurses’ willingness to engage in conversations about workarounds and patient safety.
Background: Medication Management and Technology
Medications play a critical role in the effective care of patients. Prescribing, verifying, dispensing, storing, and administering medications are all protected acts, often with specific sub-processes, which healthcare professionals spend numerous hours perfecting to ensure patient safety. However, many variables affect the outcome of the medication management process and can lead to medication errors. Medication errors are defined as “any preventable event that may cause or lead to inappropriate medication use or patient harm while the medication is in the control of the healthcare professional, patient, or consumer” (Shah et al, 2016, p. 394). These often lead to adverse drug events or “any undesirable experience associated with a patient’s use of a drug” (Shah et al, 2016, p. 394). In addition to the obvious risk to the patient’s wellbeing, medication errors and adverse drug events also accrue significant costs to the healthcare system (Bhatti, 2019).
Closed Loop Medication Management [CLMM] is a method of quality assurance and the “gold standard” in medication safety since the 1990s. Accreditation Canada, the national health organization regulatory and quality assurance board, has included various standards which encourage healthcare organizations to implement EHR and CLMM technology to ensure comprehensiveness and consistency (Accreditation Canada, 2021). For example, Accreditation Canada places particular importance on confirming two patient identifiers as part of confirming “the right patient” and has made this a Required Organizational Practice (ROP), which means health organizations must have this practice in place to increase patient safety and minimize risk (Accreditation Canada, 2021). The practice of verifying the seven medication rights is classified as a “high priority criteria” within the Medication Management Standard, signifying the importance of the criteria as it relates to patient safety, risk management, and quality improvement (Accreditation Canada, 2021).
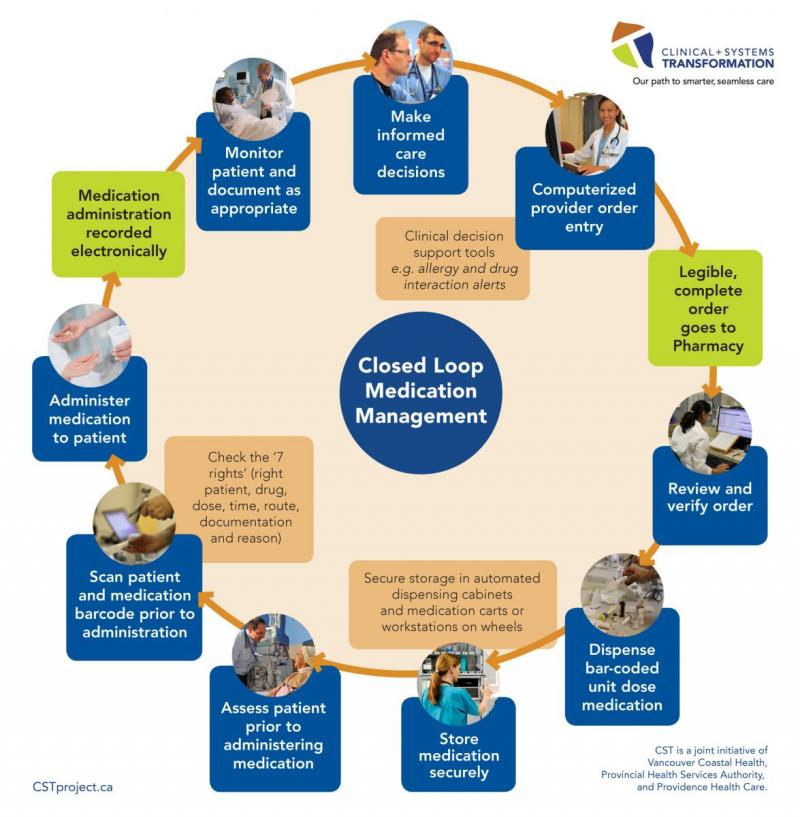
In an electronic CLMM workflow, every step in the medication management process is connected via instant documentation, and every clinician can seamlessly review what other clinicians are doing as they are doing it. Integrated electronic systems also offer various safety enhancements in the form of alerts which flag allergies, medication maximum dosages, medication incompatibilities etc. Figure 1 below outlines CLMM in more detail.
Figure 1: CLMM workflow
Background: BCMA and Workarounds
As noted above, the act of medication administration has its own specific sub-processes to ensure safety and accuracy. Nurses (Registered Nurses [RNs], Licensed Practical Nurses [LPNs] and Registered Psychiatric Nurses [RPNs]) are most often responsible for this step. BCMA represents the last portion of the medication management process when the patient finally receives the medication.
BCMA systems consist of handheld scanning devices, barcoded medication packaging, BCMA compatible computers, a barcoded patient identification (ID) band and (sometimes) a barcoded staff ID, all of which are connected to the electronic medication administration record [eMAR] and the integrated pharmacy medication manager application. Essentially, scanning each medication and the patient ID is an automation of five mediation rights: right patient, right drug, right dose, right route, and right time (Koppel et al., 2008; Shah et al, 2016). In most cases the RN utilizes a workstation-on-wheels [WOW], which includes the BCMA-compatible computer that is brought to each patient bedside to complete the scanning process. At the study hospital, there were wall mounted BCMA WOWs next to the bedside of many patients. The “right documentation” is automatically updated by following BCMA steps and typing directly into the eMAR. Despite scanning, the nurse remains responsible for all medication rights; however, the barcode scanner acts as a reliable second check. Medication rights (such as “right reason”) as well as ensuring proper medication health teaching, pre-administration assessment and monitoring post administration, are also important nurse responsibilities (BCCNM, 2010).
There is no question in the literature that BCMA systems, when used correctly, lead to a significant decrease in medication administration errors and adverse drug events, the results of which can range from unnoticeable to deadly (Shah et al, 2016, van der Veen et al, 2020). Specifically, Shah et al. (2016) found that dosing errors, incorrect medication, and wrong route errors were all decreased with the implementation of BCMA workflows in organizations which already utilized Computerized Provider Order Entry [CPOE] and Automated Dispensing Devices [ADDs] – the other technologies and sub-process employed in the CLMM workflow. A study regarding EHR implementation in mental health settings found that CLMM not only reduced medication errors, but “medication plans were also more efficient and effective because information on the therapeutic effects and medication side effects was given when the medications were prescribed or changed” (Kweon and Lee, 2021, p. 592). Additionally, it was noted in the mental health setting that overall expenses decreased, because the need for restraints and seclusion were reduced due to improved medication management (Kweon and Lee, 2021).
Therefore, it is unsurprising to learn that BCMA workarounds have been found to lead to a significant increase in medication administration errors (Truitt et al., 2016; van der Veen et al., 2017). A study published in the Annals of Pharmacotherapy conducted direct observational studies and found an average of three nursing workarounds per medication administration (Miller et al, 2011). In fact, Koppel et al (2008) identified 15 distinct types of nursing BCMA workarounds in their mixed method review of five US hospitals.
However, not all workarounds are dangerous or undesirable. Some can represent creative innovations which improve workflows (Widemen et al, 2005), and sometimes workarounds are needed to fix the “flawed” electronic system. At a minimum, workarounds can act as a flag for health leaders to signal the need to re-align frontline workflows and new HIT (Kweon and Lee, 2021).
Despite this, adverse events caused by workarounds continue at concerning rates. While the literature has revealed various insights into BCMA workaround causes, there have not been any measurable improvements in workaround rates (Seaman and Erlen, 2015). As recently as 2017, a Netherlands study found that 62% of observed BCMA medication administrations involved one or more workarounds (van der Veen et al, 2017).
Background: BCMA Workaround Causes
There are several reported causes of workarounds from a nursing perspective, including inflexibility, time pressures, workload and situational awareness, leadership, organization culture, and readiness for change (van der Veen et al, 2020). Among the cited examples of inflexibility in the BCMA workflow and eMAR are the standardized settings, which are unable to be quickly adjusted for patient preference or individualized care plans, as well as the inability to adjust for “common failures”, or the occasional expected technical glitch (Debono et al., 2013; Seaman and Erlen, 2015). These situations require users to develop workarounds to document medication administration in the eMAR correctly (Debono et al., 2013). Time pressures experienced by nurses include common HIT issues such as poor connectivity, frequently malfunctioning equipment, lack of available equipment (e.g., only two to three WOWs per unit but multiple nurses), non-portable equipment (e.g., WOWs are large and difficult to move) and poor integration of BCMA system into the existing infrastructure (e.g., the medication room is on the opposite end of unit from the BCMA WOW charging stations). All of these are viewed by nurses as “time wasters” and thus create additional time pressure when nurses follow the recommended workflow (Seaman and Erlen, 2015; Patterson, 2018).
Additionally, while BCMA may automate five medication rights, it does not provide any situational awareness necessary to manage competing priorities (Patterson, 2018). The nurse may be handling four to five patients, often with medications due at the same time, while balancing unit, hospital, and environmental factors. Unfortunately, if the BCMA (or any HIT) does not help reduce workload, it adds to the workload, thus leading to reduced compliance (van der Veen, 2020).
Leadership teams that treated noncompliance as constructive feedback saw improved BCMA uptake (Debono et al, 2013, Koppel et al, 2008, Wideman et al, 2005). Particularly, the ability for direct care staff to give anonymous feedback about BCMA workflows to leadership was found to improve BCMA use (Wideman et al, 2005). These approaches addressed the fact that most nurses are well aware that both BCMA and eMAR systems can “audit” for nonconformity, and the perception that noncompliance will be “reprimanded”, “punished” or “risk [the nurse’s] reputation” which has led to various workarounds which cause the monitored activity (i.e., scanning the medication on time) to be prioritized highly (Patterson, 2018). This is categorized as “gaming”, where a user “pretends” to follow the formal workflow steps, to avoid repercussions. A common example exists where nurses “trick” the system by scanning extra medication labels and/or patient ID bands, thus documenting a medication administration when the nurse did not yet give the medication. Gaming is often seen hand-in-hand with workarounds, but it is not a workaround in and of itself, as the sole purpose of the gaming is not to save time, but to avoid “being caught.” In fact, gaming practices often introduce more steps than the recommended workflow originally intended. Gaming behaviours and associated workarounds reflect a distrust by direct care staff towards their leadership team.
The culture of individual care units and an organization’s overall “culture of safety” also play an influential role in the attitudes of direct care nurses towards new processes like BCMA (Debono et al., 2013; ISMP Canada, 2013). The nursing profession has fought hard for professional autonomy, emphasizing patient choice, and a scope of practice that includes critical thinking in the moment – all things that are not easily achieved in the standardized design of BCMA processes (Debono et al., 2013, ISMP Canada, 2013). While some workarounds may be innovative patient-centered improvements, they are still technically workarounds and are therefore kept “under the table” by nurses in some healthcare organizations. (Koppel et al., 2008, Seaman and Erlen, 2015; Berlinger, 2017).
A scoping review by Fraczkowski et al. (2020) described causal factors for some BCMA workarounds, including “organizational un-readiness”, noting that the lack of EHR-updated policies, procedures and shared understandings with other health care providers (particularly physicians) significantly contributed to the development of nursing BCMA workarounds.
Purpose
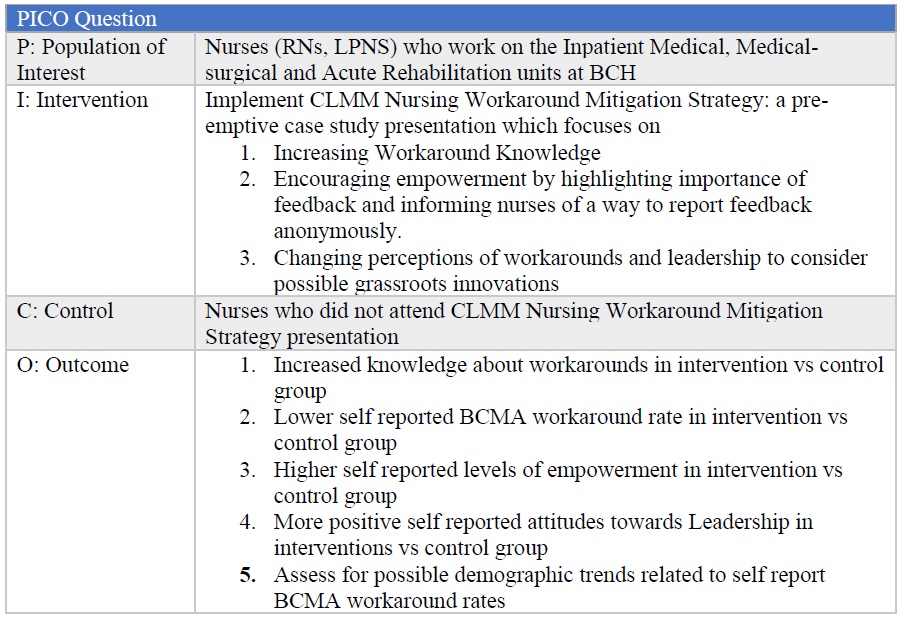
Considering the immense risk to patient safety BCMA workarounds can present, and the difficulties faced by healthcare organizations with BCMA adoption (Shackleford and McGrogen, 2021), the study site created a risk mitigation strategy, supported by clinical practice leaders within the organization, called the CLMM Nursing Workaround Mitigation Strategy. See Table 1 for full PICO question.
Table 1 – Project PICO Question
Methods
The CLMM Nursing Workaround Mitigation Strategy utilized a QI Plan Do Study Act (PDSA) cycle framework, with the primary intervention being a CLMM Nursing Workaround information session.
Information session components
The CLMM Nursing Workaround information session included a case study, information on workarounds, discussion about workarounds, examples of positive impacts from workarounds, and contrasting workarounds and gaming behaviours. The session also underlined the importance of providing feedback regarding new CLMM and BCMA workflows to leadership. The case study involved an adverse drug event in a female toddler, and storytelling techniques were used, with the context tailored to match common day-to-day situations which arise at the study site. The full Information Session PowerPoint is available at this link.
Information on workarounds
Facilitated discussions focused on defining workarounds and common causes of BCMA nursing workarounds, as well as making the distinction between workarounds and “gaming.” The session facilitator asked participants to consider the root causes of workarounds, and answer questions based on the information they just received (e.g., “What was the workaround and what was the gaming behaviour in the Case Study?”, “What were the root causes of the adverse drug event in the Case Study?”, “What could the nurse have done differently?”).
Workarounds flag a need for change
The session facilitator noted that nurses who utilize workarounds are not necessarily negligent, but often the opposite – nurses who are trying to meet the needs of their patients, and their unit at large, in a timely manner. Participants were encouraged to provide feedback on workflow processes which contribute to workarounds and were encouraged to utilize critical thinking skills to try to identify the “root cause” of the workaround and provide feedback. This concept stems from the historic QI report “To Err is Human” from the Institute of Medicine (2000), which recognizes the environmental and systemic contributors to healthcare errors.
Workarounds versus Gaming
The facilitator clarified the distinction between workarounds and gaming, noting that gaming behaviours can include inaccurate or untrue documentation, posing serious risks to patient safety. The discussion noted that while workarounds can be innovative and may lead to improvements, gaming behaviour adds no such value to the patient or to the nurse, who can easily be confused by their own imprecise charting, because gaming inevitably leads to difficulty capturing true clinical events in chronological order. Finally, the facilitator emphasized that gaming is the result of fear or mistrust between the nurse and their leadership team, and encouraged nurses to reflect on why they may be participating in gaming behaviours and supporting them to provide feedback instead. The presentation emphasized that workarounds developed at the point of care can be innovative improvements to system limitations.
Encouraging Feedback
The facilitator encouraged feedback during the session, noting that providing feedback to leadership was an essential preventative action the case study protagonist could have taken to avoid patient harm. Participants were encouraged to have their innovative workarounds “vetted” by their organization’s Professional Practice Office, to ensure the workaround was safe from all perspectives.
Session components encouraged a culture of partnership in change, in which the direct care nurses would feel empowered to not only accept the change but to participate in it via critically evaluating the new workflows and communicating their conclusions back to leadership.
Information session
Content of the Information Session was created by one author (HP) and endorsed by unit leadership at the study site. In order to attract as many direct care nurses as possible, in-person sessions were chosen, and were attached to existing Workflow Reviews (“WFRs” – Peer Mentor-led EHR sessions) to capture nurses who were in-person and on site but not providing direct patient care. The project information sessions were offered with a selection of free snacks and coffee, taking on a “Lunch and Learn” modality. Additionally, the sessions were offered in alternating unit conference rooms, all situated close to the unit staff rooms, where both on-duty nurses and nurses attending WFRs go to have lunch, so that nurses could attend the information session and still maintain appropriate COVID-19 distancing to eat lunch.
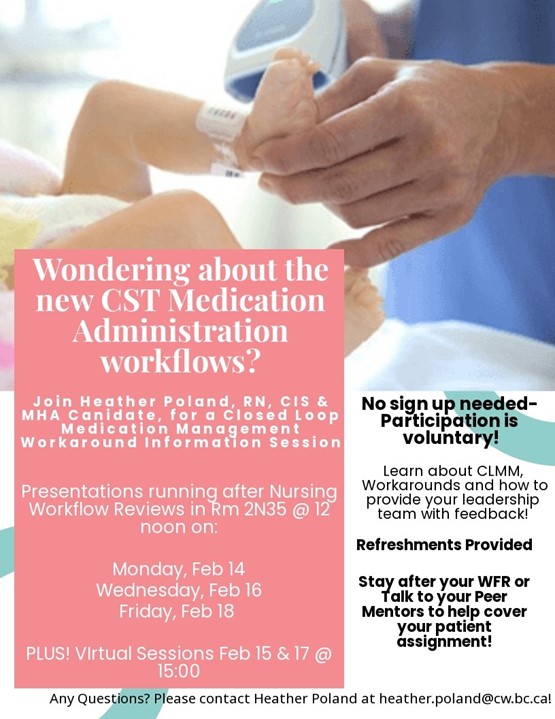
Six information sessions were offered in total, over the course of one week. The information sessions were advertised via posters placed in unit staff rooms, and on Education Boards (Figure 2). The Inpatient Educators also sent out the poster as part of their weekly updates for the month.
Figure 2: Information Session Posters
Evaluative Measures
To evaluate the impact of the information session, surveys and interviews were conducted.
Pre and Immediate Post Survey
A Pre and Immediate Post Survey was incorporated into the information session itself and was utilized to measure the extent to which the information session affected workaround knowledge, level of reported empowerment to give feedback, and attitudes toward leadership. Level of empowerment and attitudes towards leadership were markers for unit culture and were hypothesized to be susceptible to influence by a pre-emptive mitigation strategy. Limited face validity testing was conducted on survey questions with seven colleagues representing multiple professions. The wording of some questions was adjusted based on feedback. The survey was available via a QR code.
The first half of the survey – the “pre” survey – was administered before the case study and discussion. The survey was then “paused” (i.e., participants were asked to put down their phones where the survey was displayed) as the group worked through the session. The survey was picked back up at the end of the presentation and participants were asked to complete the second half of the survey – or “immediate post”- survey. The survey is available at this link.
Because the Pre and Immediate Post survey was technically one survey, there was no need to collect any identifying information to “match” pre and post information session responses. Basic information, such as nursing designation, age, home unit, employment status, and number of years nursing were collected to allow for investigation into possible demographic trends. Participants were also asked to self-report workarounds before EHR implementation. Many of the questions in the “pre” portion of the survey were directly replicated in the “immediate post” portion of the survey, allowing for a paired T-test analysis of these responses. The paired T-test was applied to each “before” and “after” question individually to determine whether differences in the results were statistically significant.
Two Month Post-EHR Implementation Survey
A second survey was developed and introduced two months after the study site completed implementation of their EHR. This Post-Implementation survey assessed longevity of changes seen in the Pre and Immediate Post Survey and allowed for a comparison of responses between the “intervention” group – the nurses who participated in the information session – and the “control” group – the nurses who did not attend the information session.
Many of the Post-Implementation survey questions were reproduced from the Pre and Immediate Post Survey, allowing the authors to determine, at a sample level, whether the information session had any lasting changes on the participants who also completed this second survey. For example, the knowledge questions in the Post-Implementation survey were closely replicated from the Pre and Immediate Post Survey, to discover if the intervention group had, firstly, remembered what they learned in the information session and secondly, if they were now more knowledgeable about workarounds than their “control group” co-workers. Limited face validity testing was again undertaken on new survey questions with the same group of colleagues. Minimal feedback was received.
The Post-Implementation survey also included open-ended questions, offering participants the opportunity to provide free text explanations to some questions. Despite the addition of qualitative questions, the Post-Implementation survey was purposefully short with a total of 21 questions (aimed to be completed in 10 minutes). The survey was advertised using a poster placed around the inpatient units and included in Weekly Updates by the Nurse Educators (See Figure 3). Additionally, a chance to win a gift card was offered to encourage participation. The Post-Implementation survey is available at this link.
Figure 3: Post-Implementation survey Poster

Qualtrics Stats iQ technology was utilized to analyse the survey results, including application of a Chi Square test. Demographic information was compared to the quantitative responses to investigate any trends. Survey responses were also examined to determine whether the participant had attended the information session or not and discern statistically significant variation between the “intervention” and “control” groups.
Interviews
Interviews were conducted with a subset of information session participants approximately three months post EHR implementation. The interview consisted of five questions with additional questions added depending on the interviewee’s responses. The interviews explored the experience of direct care nurses and their perspectives of the new CLMM and BCMA workflow and assessed whether the information session had affected any of the participants’ experiences with CLMM, workarounds or attitudes towards giving feedback to leadership.
Due to issues with low recruitment, interview invitations were also extended to those who did not complete the information session. The interview questions were adjusted accordingly. Interview transcripts were analyzed to identify common themes and concepts. The mix of “intervention” interviewees and “control” interviewees allowed for comparison of the responses between nurses who attended the information session and those who did not. The interview guide for both groups is available at this link.
Results
Pre and Immediate Post Surveys
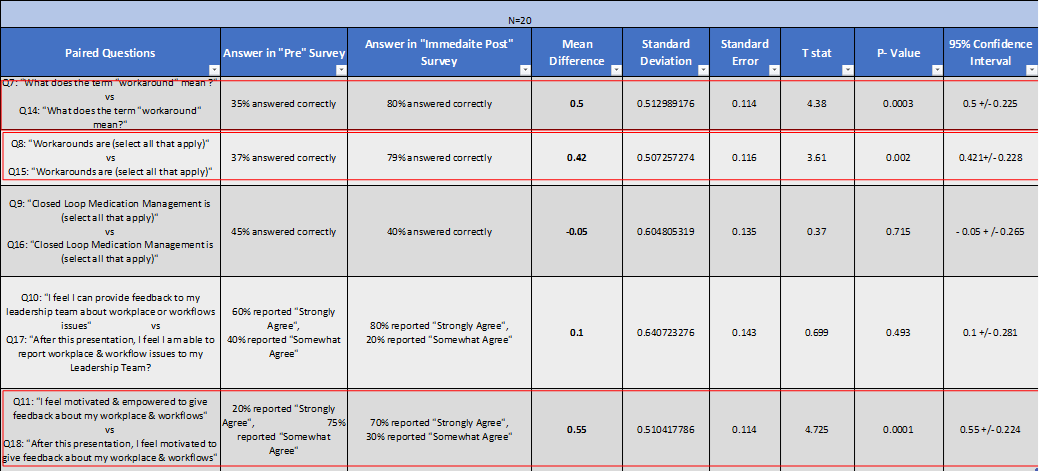
A total of 20 participants attended the information sessions and took part in the pre and post survey. There were five sets of questions in which a paired T-test analysis was conducted. Results were reported as statistically significant if the p value was less than 0.05 (see Table 2).
Table 2: Pre and Immediate Post Survey Data Analysis
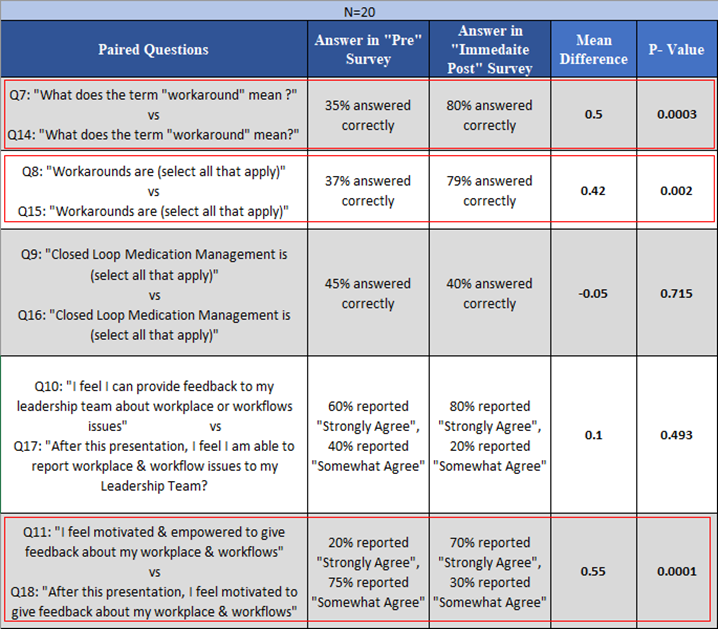
Table 3 offers the full statistical analysis. There were no statistically significant relationships found between home unit, number of years nursing, employment status, age or nurse designation and the Immediate Post survey responses.
Table 3: Pre and Immediate Post Survey Data Analysis (complete)
Two Month Post EHR Implementation Survey
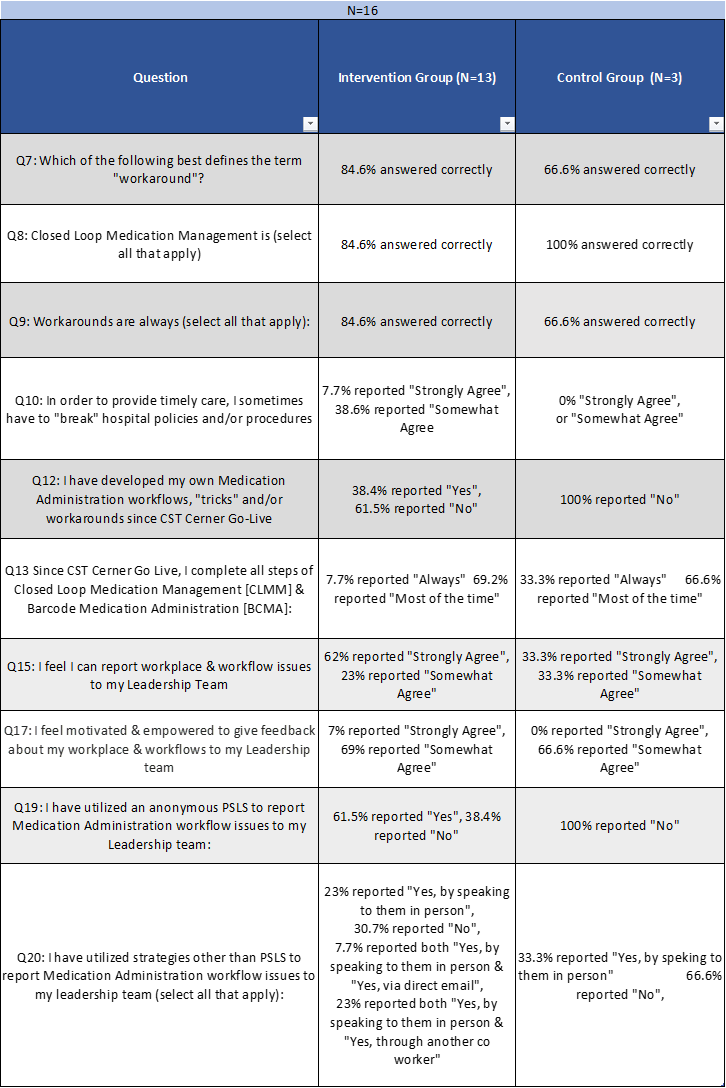
The Post-Implementation survey was completed by a total of 16 nurses, including three “control” participants who did not attend the original information session and 13 “intervention” participants who did attend the information session. This small and uneven participant group limited statistical testing reliability.
Responses related to nurses’ relationship with leadership and level of empowerment to provide feedback (markers of organization culture) indicated that 75% of respondents “strongly agreed” or “somewhat agreed” with the statement “I feel I can report workplace and workflow issues to my Leadership Team” and 69% of total respondents reported they “strongly agreed” with the statement “I feel motivated and empowered to give feedback about my workplace and workflows to my Leadership team”. Of those who reported providing feedback to leadership, 40% provided the feedback via in-person communication. Additionally, 30% of respondents reported they utilized PSLS to anonymously report workflow issues. At the time of the survey, approximately one-third of respondents reported actively engaging in workarounds.
Overall, 85% of the intervention group correctly understood that workarounds are not always negative vs 66% of the control group. The intervention group was also more likely to have given feedback to leadership, compared to the control group, and 38% of the intervention group reported utilizing the patient safety system to give anonymous feedback, contrasting to none of the control group. Eighty-five percent of the intervention group responded “somewhat agree” or “strongly agree” with the statement “I feel I can report workplace and workflow issues to my Leadership Team” compared to 66% of the control group. (see Table 4).
Table 4: Two Month Post Go Live Survey: Control vs Intervention Group analysis
Questions 10, 12, 13 and 14 had associated qualitative follow-up questions. Additionally, the final survey question offered space for a free text response to “Is there anything else you would like to say about the new EHR medication administration workflows”. Table 5 describes the qualitative feedback collected via the Post-Implementation survey.
Table 5: Qualitative Feedback collected from Post-Implementation Survey
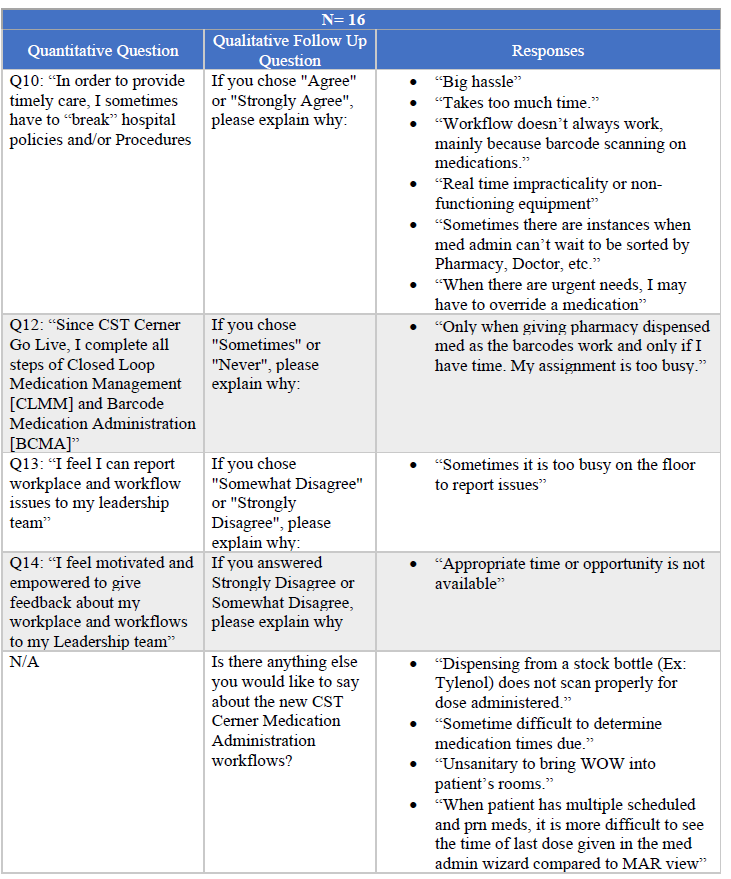
Three major themes can be extracted from this data: 1) time pressure was experienced by many of the respondents making it difficult to adjust to the new workflows; 2) technical issues, particularly with barcodes, prevented accurate scanning (e.g.: “Dispensing from a stock bottle (Ex: Tylenol) does not scan properly for dose administered”); and 3) the new “view” of the MAR on the EHR is not as clearly understood as the previous paper MAR (e.g., “Sometimes it is difficult to determine medication times due”).
Pre and Immediate Post Survey vs Post-Implementation Survey
One of the main goals of the Post-Implementation survey was to assess for longevity of the changes noted immediately after the information session. The same five questions which were replicated from the “pre” survey to the “immediate post” survey were utilized in the Post-Implementation survey, allowing the authors to track trends of the ‘intervention” group who had attended the information session and (presumably) completed the Pre and Immediate Post Survey. To maintain anonymity of participants, the Post-Implementation surveys were not matched to the original Pre and Immediate Post survey. Table 6 summarizes the findings.
Table 6: Longevity of learning between Immediate Post Survey and Post-Implementation Survey
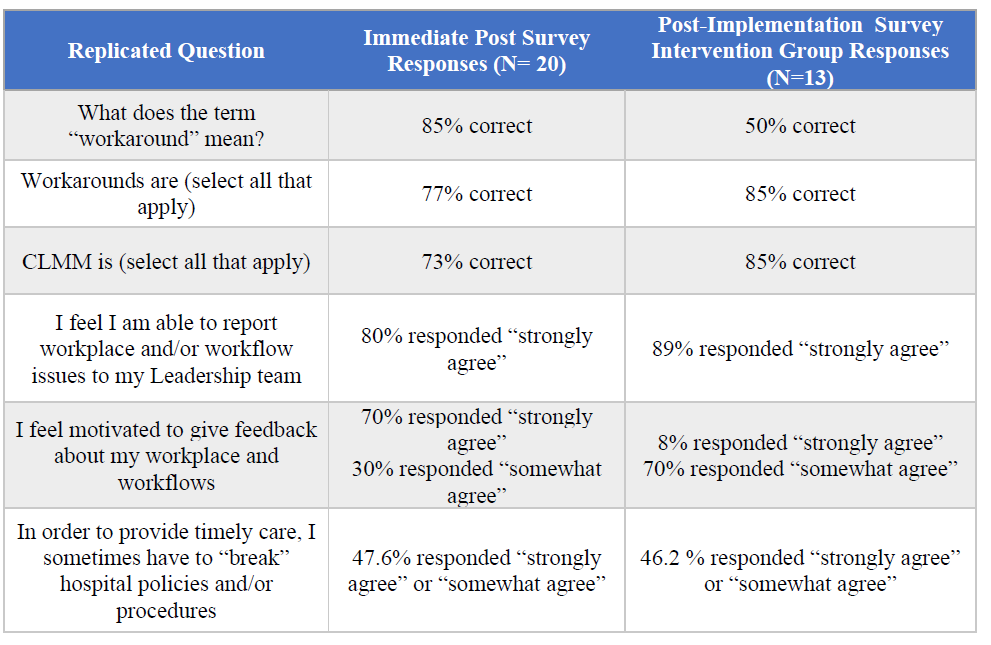
Of note, there was a decreased understanding of the definition of workarounds, but an increased appreciation of what CLMM entails and the idea that workarounds are not always negative. There were also increased feelings that participants could report workplace or workflow issues to the leadership team. While more participants reported “I feel I am able to report workplace and/or workflow issues to my leadership team” there was a slight decrease in motivation to provide feedback, with 100% of Pre and Immediate Post survey participants reporting “strongly agree” or “somewhat agree” as compared to 85% of intervention groups with the same responses to the same question in the Post-Implementation survey. Similarly, in the Pre & Immediate Post survey, 85% of participants stated they “strongly agreed” with the statement “After the presentation, I am likely to report workplace or workflow issues”; however, when asked if they provided any type of feedback, only 70% of the intervention group responded “yes”. Of that 70%, approximately 39% provided feedback via the anonymous patient safety reporting system approach presented in the information session.
Interviews
In total, five interviews were conducted. The interviews were analysed for common themes. Three major concepts emerged:
“It’s harder than it sounds”
This theme was found throughout the five interviews, regardless of whether the interviewee had attended the information session. In general, all the interviewees spoke about “pressure” to get things done on time and difficulty balancing the new BCMA requirements with other things to do, such as “bedside procedures, talking to patients, talking to doctors, etc.” (Interview #1). The workflow for stock medications, such as children’s acetaminophen (extremely common medication given throughout study site hospital), came up specifically in four out of five interviews. The interviewees all found it “annoying” or “not ideal” to have to leave the stock medication bottle, e.g., acetaminophen bottle, in the medication dispensing unit, for the sole purpose of being able to get a printed label to allow CLMM, which even when scanned, still requires the nurse to edit the medication dose amount – because the label indicates the nurse is giving the patient a full acetaminophen bottle (Interview #1, #3, #4, #5). Similar “clunky” workflows were described for crushing medications and for “Care by Parent” workflows.
A second factor which made BCMA workflow “harder than it sounds” was around technical issues or drawbacks, such as scanning the patient wristband during night shift. All interviewees reported that no one wanted to wake a sleeping child to scan the patient’s ID band and there was visible evidence of nurses printing out an extra patient ID label and sticking it to the WOW computer at the patient’s bedside to avoid having to disturb the patient to get to the wristband. Interview #1, #2, and #4 also noted that originally no one knew how to reduce the volume of the scanner, which led to very loud beeping every time the nurse scanned anything, thus disturbing patients and families. The solution for this was found relatively quickly via Cerner technical “elbow support”, but the experience “made a lasting impression on the floor”. Additionally, while all the interviewees felt that BCMA was inarguably “safer”, they noted that colleagues were skeptical about the need to scan the wristband to identify the patient, particularly when the patient was “long term” (Interview #5). Issues with barcodes not scanning was also brought up in multiple interviews (Interview #2, #3, #5). This includes initial confusion with some medications not having a barcode at all and some medication barcodes simply not working. For example, the barcode scanner on some inhalers notoriously did not work, presumably because the barcode is wrapped around a small inhaler cylinder (Interview #1). These situations led to confusion, with some nurses unclear if they were supposed to “troubleshoot” or if they should just be calling pharmacy (Interview #2) and this led to increased stress and “reactivity” (Interview #3). Additionally, Interview #3 noted that there was confusion around the number of “alerts” nurses must click through, with reports of increased “pop up fatigue” and feelings that some pop ups seemed unnecessary.
Finally, Interview #1 and #5 reported feeling “guilty” or “ashamed” that they did not have more empathy for direct care nurses when they worked as Peer Mentors because they found the BCMA workflows difficult when they were back at the bedside themselves.
Open discussions about workarounds
This theme was reported by all the interviewees who attended the information session. Interviewee #1 reported that “knowing there was a shared understanding of workarounds and gaming [between the information session participants] makes it easier to approach them”, “if leadership was verbalizing that workarounds were all bad, it would make it harder to talk about” and “if I didn’t know that my leadership team was open to assessing and listening and understood the intricacies of workarounds, I would be more likely to do gaming behaviours”. Interview #2 noted that the information session brought workarounds “to the forefront, as it had not been a topic of discussion before”. According to Interviewee #2, “there hadn’t been any changes to the [medication administration] workflow for so long” and that the unit had been relying on the patient safety reporting system and dealing with issues reactively on a one-by-one basis. The information session allowed Interviewee #2 to “reflect on why workarounds happen and to be cognisant that there are many system reasons for workarounds – like the scanner not working”. Finally, Interviewee #3 noted an “increased capacity to discuss workarounds as possible solutions” and said, “I was so narrow minded before. The idea of workflow [issues] makes so much sense… it’s not always the nurse’s choice or decision or laziness, sometimes it’s a systems adaptation”. Interviewee #3 also stated that the information session “put a conversation on something we all knew was happening… I appreciated dedicated time to think about it and was able to have specific conversations about workarounds on the floor” because of that reflection time.
The interviewees who did not attend the information session reported different experiences discussing workarounds. Interviewee #4 reported feeling open to discussing workarounds but didn’t have actual conversations about them. Interviewee #5 reported that “we have a culture where we do it our way, then if leadership is close by, we do it the proper way” and felt that “I can’t think of a better way to do it, so I felt that I couldn’t [give feedback] even though I know the workflow isn’t going as planned.”
Helpful for teaching
This concept was touched on by all the interviewees who attended the information session. Interviewees felt that the increased awareness about workarounds being the result of systems issues and possibly even positive adaptations, made it easier to take advantage of “teachable moments”. Interviewee #2 stated they would ensure they addressed the issue of workarounds when teaching BCMA processes at subsequent WFRs. Interviewee #3 noted that much of the support given as a Peer Mentor was for medication administration and that they were able to have multiple discussions about workarounds and even noted some “safe” workarounds which still met CLMM requirements. Interviewee #1 said, “The case study was helpful because it emphasized the importance of BCMA workflows and gave an example which helped me illustrate how [BCMA] helped things.” Nevertheless, interviewees noted that there was some uneasiness around how hard to push “the rules” during the first months post EHR implementation, and a feeling that Peer Mentors and the leadership team had to “pick our battles”. Interviewee #2 noted “staff who work at other hospitals already knew all the workarounds and they seemed to spread like wildfire”. Interviewee #5 felt “workarounds were going to happen regardless” and so did not put too much pressure on trying to correct them, stating “if they [direct care nurses] did it in front of me I would say ‘I’m going to pretend you didn’t do that”.
Discussion
The events of the past two years, including the stresses on healthcare staff caused by the COVID-19 pandemic, increased violence towards healthcare staff, a medication negligence legal case against a nurse, RaDonda Vaught, in the US (Lotter, 2022; Landman, 2022), increased evidence of systemic racism within the Canadian healthcare system, and a precedent-setting salary cap for nurses in Ontario, have led to a heightened distrust by direct care nurses of their leaders. These events highlight the need to focus on strengthening organizational culture and building trust between direct care staff and their leaders, to promote successful adoption and sustained appropriate use of CLMM and BCMA, and thus promote patient safety.
Results from this study illustrate that BCMA workarounds are rampant, beginning and spreading quickly upon EHR implementation. Relying on adverse event investigations to “prove” that workarounds are a dangerous reality is a reactive approach to an issue that cannot be easily remediated. As noted above, workarounds can act as a flag for healthcare leaders, signalling a need to re-align workflows and address nursing concerns, and we urge healthcare leaders to initiate ongoing conversations and education with their direct care nurses, to support a culture of openness about workarounds and patient safety concerns.
Providing nurses with clear definitions, developing shared understandings and emphasizing the organization’s process of sharing feedback and collective problem solving is vital for creating clear, accessible and open communication between direct care nurses and leadership. Nursing baccalaureate programs also have an opportunity to address workarounds and CLMM within their curriculum and thus communicate these introductory concepts to nurses early on in their careers.
This project illustrated that a relatively simple intervention can have a meaningful impact on medication safety within an EHR. Participation in the intervention led to a significant increase in nurses’ understanding of workarounds and motivation to discuss them openly with leadership.
We encourage healthcare leaders to invest in informational sessions regarding CLMM and nursing workarounds, during EHR implementation and in new nursing staff orientation. Doing so would indicate to staff that their leaders are open to workaround discussions and want to receive feedback, thus promoting a culture of partnership in change, including open transparent conversations between unit leadership, professional practice, and direct care clinicians. Furthermore, it is recommended that organization leadership teams develop, implement, and study the usage of an agreed-upon strategy to allow direct care staff to submit anonymous feedback regarding workarounds.
The result of this innovative and relatively low-cost project indicates that further investment in preventative workaround mitigation strategies are warranted, specifically in healthcare organizations utilizing EHRs. While it may be impossible to completely stop workarounds, creating an organizational culture where patient safety and nurses’ feedback are valued is fundamental.
Limitations
This project faced various limitations, including a small sample size for the surveys, and a high attrition rate from the pre-implementation information session to the post-implementation and interviews, making comparisons difficult.
Author Biographies
Heather Poland, RN. BScN, MHA
BC Children’s & Women’s Hospital, Heather.Poland@cw.bc.ca
Heather is a Paediatric RN and Clinical Informatics Lead working with the CST Project in the Lower Mainland, BC. She received her BScN from Western University in Ontario before moving to BC. Recently she graduated from the Master of Health Administration program at the University of British Columbia in Vancouver.
Agnes T. Black, RN MPH
Providence Health Care, ablack@providencehealth.bc.ca
Agnes is the Director, Health Services & Clinical Research and Knowledge Translation. She completed her BSN at the University of Washington, Seattle, and her Master of Public Health at Simon Fraser University. She is an adjunct professor at the University of British Columbia School of Nursing and Research Associate, Centre for Health Evaluation & Outcome Sciences.
Isabel Diogo, RN, BScN, MScN
Providence Health Care, idiogo@providencehealth.bc.ca
Isabel is the Practice Consultant, Medication Safety and Management within the Professional Practice Department. She completed both her BScN and MScN degrees at the University of British Columbia. She has experience and interest in mental health, operations, medication practice, clinical informatics, quality improvement and patient and family centered care.
References
Accreditation Canada. (2021). Medication Management Standards. https://store.accreditation.ca/products/medication-management-standards
BC Children’s Hospital (2022) History. http://www.bcchildrens.ca/about/history
Berlinger, N. (2017) Workarounds Are routinely used by Nurses-But are they ethical? The American Journal of Nursing, 117(10), 53–55. doi: 10.1097/01.NAJ.0000525875.82101.b7.
Bhatti, A. (August 8, 2019). Adoption of closed loop medicines administration into the NHS. The Pharmaceutical Journal. https://pharmaceutical-journal.com/article/opinion/adoption-of-closed-loop-medicines-administration-into-the-nhs
Booth, R. G., Sinclair, B., Strudwick, G., Hall, J., Tong, J., Loggie, B., Chan, R. (2017) Chapter 12 – Strategies Through Clinical Simulation to Support Nursing Students and Their Learning of Barcode Medication Administration (BCMA) and Electronic Medication Administration Record (eMAR) Technologies, ethics.In Shachak Aviv, Elizabeth Borycki, Shmuel P. Reis (Editors). Health Professionals’ Education in the Age of Clinical Information Systems, Mobile Computing and Social Networks. Academic Press, pp 245-266, doi: 10.1016/B978-0-12-805362-1.00012-7.
British Columbia College of Nurses and Midwives [BCCNM]. (2010). Practice Standard for Registered Nurse and Nurse Practitioners: Medication Administration. https://www.bccnm.ca/Standards/RN_NP/PracticeStandards/Lists/GeneralResources/RN_NP_PS_MedicationAdmin.pdf
Buerhaus, P. I. (2013). Human factors engineering, bar coding medication administration, and Nursing: An interview with Drs. Richard Holden and Laurie L. Novak. Nursing Economic$, 31(4), 190–197.
Burkoski, V., Yoon, J., Hutchinson, D., Solomon, S., & Collins, B. E. (2019). Experiences of Nurses working in a fully digital hospital: A Phenomenological study. Nursing Leadership 32(SP), 72–85. https://doi.org/10.12927/cjnl.2019.25813
Canada Health Infoway (2022) Electronic Health Records: Transforming healthcare, improving lives. Corporate Business Plan 2007-08.
Debono, D.S., Greenfield, D., Travaglia, J.F., Long, J.C., Black, D., Johnson, J., Braithwaite, J. (2013) Nurses’ workarounds in acute healthcare settings: a scoping review. BMC Health Services Research, 13(1), 1–16. doi: 10.1186/1472-6963-13-175.
Fischer, D. (2019). Storytelling as a Nursing pedagogy. The Midwest Quarterly, 60(3), 311–318.
Fraczkowski, D., Matson, J., Lopez, K. D. (2020)Nurse workarounds in the electronic health record: An integrative review. Journal of the American Medical Informatics Association, 27 (7) pp 1149–1165, https://doi.org/10.1093/jamia/ocaa050
Institute of Medicine, Committee on Quality of Health Care in America. (2000). To Err Is Human: Building a safer health system. National Academies Press.
ISMP Canada. (2013) Medication bar code system implementation Planning: A resource guide. https://www.ismp-canada.org/barcoding/download/ResourceGuide/BarCodingResourceGuideFINAL.pdf
Koppel, R., Wetterneck, T., Telles, J.L., Karsh, B.T. (2008). Workarounds to barcode medication administration systems: Their occurrences, causes, and threats to patient safety. Journal of the American Medical Informatics Association; 15 (4) pp 408–423. https://doi.org/10.1197/jamia.M2616
Kweon, Y. & Lee, S. (2021). Nurses’ electronic medical record workarounds in mental healthcare settings. CIN: Computers, Informatics, Nursing, 39 (10), 592-603. doi: 10.1097/CIN.0000000000000762.
Lotter, T. (2022) Nurses protest Tennessee sentence for deadly medical mistake. In CTV News: health. https://www.ctvnews.ca/health/nurses-protest-tennessee-sentence-for-deadly-medical-mistake-1.5901884
Landman, K. (2022) A nurse made a fatal error. Why was she charged with a crime? How the RaDonda Vaught case threatens patient safety. In Vox. https://www.vox.com/science-and-health/23046679/radonda-vaught-nurse-medication-medical-error-patient-safety-lawsuit-vanderbilt
Milota, M. M., van Thiel, G. J. M. W., van Delden, J. J. M. (2019) Narrative medicine as a medical education tool: A systematic review. Medical Teacher, 41(7), 802-810, DOI: 10.1080/0142159X.2019.1584274
Miller, D. F., Fortier, C. R., &and Garrison, K. L. (2011). Bar Code Medication Administration technology: Characterization of high-alert medication triggers and clinician workarounds. Annals of Pharmacotherapy, 45(2), 162–168. https://doi.org/10.1345/aph.1P262
Patterson, E.S (2018). Workarounds to intended use of health information technology: A arrative review of the human factors Engineering literature. Human Factors: The Journal of the Human Factors and Ergonomics Society, 60 (3), 281-292. https://doi-org.ezproxy.library.ubc.ca/10.1177/0018720818762546
Registered Nurse Association of Ontario (2022) About the best practice champions’ network. https://rnao.ca/bpg/get-involved/champions
Seaman, J. B., & Erlen, J. A. (2015). Workarounds in the workplace: A second look. Orthopedic Nursing, 34 (4), 235–242. https://doi.org/10.1097/NOR.0000000000000161
Shah, K., Lo, C., Babich, M., Tsao, N. W., & Bansback, N. J. (2016). Bar Code Medication Administration technology: A systematic review of impact on patient safety when used with Computerized Prescriber Order Entry and Automated Dispensing Devices. The Canadian Journal of Hospital Pharmacy, 69(5), 394–402. https://doi.org/10.4212/cjhp.v69i5.1594
Shackleford, K. & McGrogan, M. (2019) BCMA to discharge huddle [PowerPoint Slides]
Schurman, S.J., Keeler, V. & Welch, T.R. Massive gentamicin overdose in a 14-month-old. Pediatric Nephrology, 24(1), 211–213. https://doi.org/10.1007/s00467-008-0941-8
Truitt, E., Thompson, R., Blazey-Martin, D., NiSai, D., & Salem, D. (2016). Effect of the implementation of barcode technology and an Electronic Medication Administration Record on adverse drug events. Hospital Pharmacy; 51(6), 474–483. https://doi.org/10.1310/hpj5106-474
van der Veen, W., van den Bemt, PMLA., Bijlsma, M., de Gier, H.J., Taxis, K. (2017) Association between workarounds and medication administration errors in Bar Code-Assisted Medication Administration: Protocol of a multicenter study. JMIR Research Protocols, 6(4), e74. Doi: 10.2196/resprot.7060
van der Veen, W., Taxis, K., Wouters, H., Vermeulen, H., Bates, DW., van den Bemt, PMLA. (2020) Factors associated with workarounds in barcode?assisted medication administration in hospitals. Journal of Clinical Nursing, 29(13–14), 2239–2250. https://doi.org/10.1111/jocn.15217
Wideman, M.V., Whittler, M.E., Anderson, T.M. (2005) Barcode Medication Administration: Lessons Learned from an Intensive Care Unit Implementation. In K. Henriksen, J.B. Battles, & E.S. Marks, Editors. Patient Safety: From Research to Implementation; Volume 3: Implementation Issues. https://www.ncbi.nlm.nih.gov/books/NBK20569/




Recent articles
- Index of volume 21 number 221 Jun 2026
- What does Canada’s new National Artificial Intelligence Strategy mean for healthcare?21 Jun 2026
- UN SDGs and Open Source Principles as Outcomes and Implementation Approach to Health Informatics21 Jun 2026
- Designing Compassionate Systems: Why Nursing Must Lead in the Age of AI21 Jun 2026
- Advancing Nursing Informatics Through the Integration of Genomics: Addressing Barriers and Capacity Building in Canadian Healthcare21 Jun 2026