
Empathy in Action: An Immersive Training Approach to Support Dementia

by Dr Eva Peisachovich, RN PhD
Dr Tin D. Vo
Dr Bill Kapralos
Dr Celina da Silva, RN, PhD
Dr Naida L. Graham, PhD
Shai S. Rahmanov
Citation: Peisachovich, E., Vo, T. D. Kapralos, B., da Silva, C., Graham, N. L, Rahmanov, S. S. (2025). Empathy in action: An immersive training approach to support dementia. Canadian Journal of Nursing Informatics, 21(1). https://cjni.net/journal/?p=16072
Abstract
The increasing prevalence of dementia worldwide underscores the urgent need for innovative, empathy-centred approaches to caregiver and healthcare professional (HCP) education. To address this, we developed the Augmented Reality Education Experience (AREduX), an augmented reality (AR) simulation that immerses users in the sensory, cognitive, and emotional challenges of living with dementia. Using a mixed-methods approach, we developed, implemented, and evaluated AREduX through a four-phase design-based process that included prototype development, usability testing, experiential workshops, and pre- and post-test assessment of empathy and care competence.
The first three phases included prototype development, usability testing, and an iteration based on data collected, while the fourth phase involved experiential workshops (Peisachovich et al., 2022). This paper presents the results of the fourth phase, which involved pre- and post-assessment of empathy and care competence. In Phase 4, 15 participants (13 HCPs, 2 caregivers) completed a structured workshop and engaged with AREduX using an AR headset and aging suit. Quantitative data were collected using the Toronto Empathy Questionnaire (TEQ) and the Sense of Competence in Dementia Care Staff (SCIDS) scale. Although TEQ scores showed no statistically significant change, SCIDS results indicated enhanced perceived competence post-simulation. Qualitative findings, drawn from field observations and focus-group interviews, revealed strong emotional responses to the simulation: Participants described the experience as frustrating, physically challenging, and deeply eye-opening. These affective reactions suggest that AREduX evoked meaningful shifts in empathic understanding that may not be fully captured by traditional self-report measures.
This study demonstrates the feasibility and experiential impact of using AR for dementia empathy training. While further research with larger sample sizes and improved measurement tools is needed, AREduX shows promise as an immersive educational intervention capable of strengthening empathy and care quality in dementia support contexts.
Background
Canada is facing a dementia epidemic that currently affects over 650,000 people and costs the healthcare system $15.1 billion annually (Alzheimer’s Disease International, 2024; Alzheimer Society of Canada, 2024; Canadian Centre for Economic Analysis, 2023). Projections indicate that by 2030, the number of Canadians living with dementia will approach one million, and the demand for long-term care will increase tenfold, raising the total annual economic burden to more than $153 billion (Alzheimer Society of Canada, 2010a). The rising prevalence of dementia in Canada reflects a broader global trend. According to the World Health Organization (2021), 57 million people worldwide lived with dementia in 2021, and this figure is estimated to reach 82 million by 2030.
Beyond the overwhelming financial implications, dementia exacts a profound human toll. People living with dementia (PLWD) often experience memory loss, depression, anxiety, isolation, and a loss of independence and identity (Alzheimer Society of Canada, 2010b). These challenges impact caregivers, who frequently face long-term physical, emotional, and financial burdens, and healthcare professionals (HCPs) who must respond to increasingly complex care needs (Canadian Nurses Association, 2016; Prince et al., 2013). As front-line service providers, HCPs serve as key sources of education and support for patients and families, underscoring the importance of specialized training to enhance understanding and care for PLWD (Home Care Ontario, 2017).
Empathy, the ability to understand another person’s feelings and perspectives, is critical to effective, person-centred care. Research shows that HCPs with high empathy levels deliver better clinical outcomes and improve patient satisfaction (Cunico et al., 2012; Dal Santo et al., 2013; Hojat et al., 2023; Keshtkar et al., 2024). In educational contexts, empathy also enhances learner engagement and information retention (Cai et al., 2023). Despite this, an evidence-based understanding of empathy in dementia care remains underdeveloped (Salazar et al., 2023; Sinclair et al., 2018; Winter et al., 2022), yet the need for innovative, immersive empathy-focused training tools for empathy building is pressing.
To address this gap, we developed the Augmented Reality Education Experience (AREduX), an augmented reality (AR) simulation designed to increase empathy by enabling users—HCPs and informal caregivers—to step into the world of PLWD. Drawing on serious game design principles and emerging AR technologies, AREduX replicates the sensory, cognitive, and emotional experiences associated with dementia, offering an experiential education approach. Grounded in Kolb’s (1984) experiential learning theory, AREduX engages partipants through concrete experiences and reflective observation, facilitating the transformation of experience into knowledge and empathyThis paper describes the development, implementation, and early impact of AREduX, offering insights into its potential as a transformative tool for empathy-building in dementia care.
In Phase 1, the development of AREduX began with a thorough needs analysis, involving focus groups, questionnaires, and interviews with HCPs, caregivers of PLWD, computer software designers, and educational developers (Peisachovich et al., 2022). These insights guided the design process, which employed the design, play, and experience framework (Winn, 2009) to ensure a formal, iterative development approach. The design aimed to simulate the sensory, auditory, visual, and cognitive impairments often experienced by PLWD (Zwijsen et al., 2016). Auditory challenges were reflected through muffled speech and distorted sounds, mimicking hearing difficulties (Hardy et al., 2016), while visual impairments were represented by blurred visuals and disorientation, simulating reduced contrast sensitivity and spatial awareness (Jones et al., 2020). Cognitive challenges were embedded through features designed to mirror the memory gaps and delayed decision-making that PLWD often encounter; the provision of incomplete, ill-timed, or overwhelming information mimicked the experience of processing memory gaps, while system lags in presenting play options or responding to player input simulated delays in decision-making and reaction times. To enhance empathy, participants also wore an “aging suit” (see Figure 1) that restricted movement and reduced sensitivity to touch, further simulating the physical effects of aging.
Figure 1
AREduX Prototype Aging Suit

In Phase 2, the fully functional AREduX prototype was subjected to a usability study. This included both quantitative and qualitative evaluations: participants (HCPs and caregivers) completed the System Usability Scale (SUS) to assess the platform’s usability—that is, the quality of the user experience, including the system’s technical performance (Sauro, 2011)—and participated in a focus-group interview, which garnered data on user experiences. The feedback collected from participants provided insight into how AREduX could be integrated into empathy-focused training in higher education curricula and continuing-education workshops. A semi-structured interview captured participant thoughts on the platform’s educational design, comprehension, and problem-solving support. The findings from these assessments not only validated the prototype but also revealed areas for refinement. Based on the feedback gathered in Phase 2, Phase 3 focused on revising and improving AREduX to better meet the needs of its intended users.
The implementation of AREduX occurred in Phase 4; AREduX was integrated into an experiential-education workshop designed for HCPs and caregivers of PLWD. The primary goal of this phase was to evaluate the impact of AREduX on participants’ empathy and awareness, using a structured, evidence-informed protocol.
Two separate workshops were developed—one for HCPs (n = 9) and another for caregivers (n = 2). Each 90-minute session was delivered in a face-to-face format and included a 60-minute educational component covering topics such as the distinctions between normal and abnormal aging, early warning signs of dementia, and communication challenges. The sessions incorporated evidence-based communication strategies that have been shown to improve care outcomes for PLWD. Given the central role of empathy in effective communication, the AREduX prototype was embedded within the workshop as an experiential-learning tool.
This phase highlighted the promise of AREduX as an experiential-learning tool that can be meaningfully integrated into both professional and informal caregiver training, contributing to enhanced empathy and improved communication practices in dementia-care contexts.
Methodology
The team employed both quantitative and qualitative methodologies through an exploratory lens guided by these research questions:
- Are end users comfortable using AREduX as an experiential education tool?
- Does AREduX enhance the empathy levels of HCPs working with PLWD?
- Does AREduX enhance empathy among caregivers of PLWD?
- Will AREduX impact the confidence levels of HCPs and caregivers when caring for PLWD?
Setup and Moderation
The workshops took place at the Ontario Shores Centre for Mental Health Sciences in Whitby, Canada. We employed a simulation-based approach aligned with best practices in HCP education, consisting of three structured phases: a pre-brief to set expectations and prepare participants; the simulation experience itself, which used an AR headset (Microsoft Hololens 2) and an aging suit to simulate how PLWD might experience tasks such as setting a table, making a sandwich, and taking a pill (see Figure 2); and a debrief to facilitate reflection, discussion, and integration of learning. Throughout the process, observational field notes were taken. After the debrief, each participant completed the TEQ and SCIDS questionnaires. A follow-up focus-group session was conducted.
The workshop began with an introductory mini lecture by a research assistant, covering dementia, the project, and the purpose of the simulation. Participants then engaged in the simulation, wearing an aging suit and AR headset. The session concluded with a debrief on the experience.
Figure 2
A Screen Capture of an AREduX Scenario

Data Collection
In order to garner sufficient numbers for analysis, we collected data at three distinct points in the project timeline: pre-implementation of the AREDuX experience, post-implementation, and during the Phase 4 focus group sessions; data for the pre- and post-implementation phases were collected through questionnaires. Once data collection was completed, quantitative data from the empathy scales were triangulated with qualitative insights from the focus groups to better understand the immediate educational and emotional impact of the simulation experience. The data collection protocol included the following steps:
Pre-Assessment: Participants completed the Toronto Empathy Questionnaire (TEQ; Spreng et al., 2009) prior to the workshop to establish a baseline measure of empathy.The TEQ represents empathy as a primarily emotional process and is a reliable and valid instrument for the assessment of empathy.
AREduX Exposure: Participants were introduced to and engaged with AREduX during the workshop session. Length of engagement with the simulation scenario varied by participant and ranged between 3 and 20 minutes.
Post-Assessment: After using AREduX, participants again completed the TEQ to measure any changes in empathy levels. Additionally, they completed the Sense of Competence in Dementia Care Staff (SCIDS) scale (Schepers et al., 2012) to assess engagement and interest in the simulation experience and to determine if AREduX, used in combination with the educational workshop, impacts confidence when caring for or interacting with PLWD.
Focus Group: Following the workshop, separate focus-group-session interviews were conducted with each participant group (HCPs and caregivers). Focus-group sessions were held online using Zoom video-conferencing software. This software was used to transcribe audio recordings of the sessions, and transcriptions were subsequently checked for accuracy by one of the researchers. During the focus-group sessions, participants answered questions regarding their experiences and opinions of AREduX. These sessions provided qualitative insights into participants’ experiences with AREduX, its perceived impact, and suggestions for future adaptation and implementation.
Participants
Participants were recruited through the Ontario Shores Centre for Mental Health Sciences in Whitby, Canada, and were associated with geriatric units at this hospital. Recruitment advertising flyers were posted in the geriatric units and emailed to subscribers to a mailing list for family members of patients. Participants were offered a $25 gift card for involvement in each stage: the workshop, with pre/post survey completion and the focus-group-session interviews.
A total of 15 participants (13 HCPs who were working in a professional capacity with PLWD and 2 family caregivers) took part in the educational workshop. Four of the HCPs who participated in the educational workshop did not attend a focus-group session due to scheduling constraints. The remaining 11 participants took part in a focus-group session to provide feedback on their experience with AREduX. This group included two family caregivers and nine HCPs (three nurses, three social workers, one behaviour therapist, one occupational therapist, and one recreation therapist). None of the participants had prior experience with AR.
Due to the exploratory nature of this study, this sample size is reasonable, particularly given that the goal was to assess feasibility, instrumentation adequacy, and preliminary trends and to provide statistical estimates for a larger study (Julious, 2005).
Following the completion of the pre- and post-survey data collection, a subset of participants (nine HCPs and two caregivers of PLWD) participated in focus groups. Two separate focus groups, one with HCPs and one with caregivers, were conducted to gather in-depth feedback on participants’ experiences with AREduX. Using a semi-structured interview format, we explored participant satisfaction with the workshop experience, focusing on the role of experiential education, the perceived benefits and challenges of embedding AREduX into professional development and caregiver training, and suggestions for further improvement.
To be eligible for inclusion in the study, participants had to be willing to complete the workshop and to take part in a focus group following the workshop. Moreover, we required that at the time of the study HCPs were working in a healthcare setting with PLWD and caregivers were formally or informally providing care to a person living with dementia. We excluded individuals with a vision impairment at a level that would make it difficult or impossible to engage with AREduX.
Observations
Paticipants found the AREduX simulation experience—in which they used an AR headset and wore an aging suit to simulate challenges PLWD might encounter when completing everyday tasks (setting a table, making a sandwich, and taking a pill; see Figure 3l)—to be both eye opening and frustrating. These tasks were designed by the team to reflect daily activities that might become challenging for dementia patients, especially those with physical, sensory, and cognitive impairments. Key observations were frustration and physical difficulty.
Figure 3
Screen Capture of Scenario of Making a Sandwich and Taking a Pill

During the table setting simulation, the HCPs frequently struggled with the basic tasks of picking up utensils, placing objects, and aligning a glass with a coaster. The AR headset and aging suit both contributed to these difficulties, as they reduced dexterity, created visual impairments, and impeded movement. Task complexity was involved as the simulation was designed to mimic the cognitive and physical challenges of dementia. Tasks that seemed simple, such as picking up a fork or arranging utensils, became overwhelming. Participants reported difficulty with coordination, grasping objects, and completing even basic movements, illustrating the emotional and physical strain of such tasks on PLWD.
The use of the aging suit was effective in fostering empathy among participants. Many HCPs reported feeling frustrated and exhausted, which allowed them to better understand why dementia patients may become agitated or disoriented when performing routine tasks. The constant sensory overload and sense of restriction of movement allowed participants to appreciate how overwhelming even small tasks can be for those with dementia. Despite the frustrations, many participants expressed a sense of pride upon completing the simulation. This sense of accomplishment mirrored the feelings that patients may experience when successfully completing a task, despite the difficulties involved. The simulation allowed HCPs to understand why patients may require repeated encouragement or assistance to complete tasks. While the simulation was viewed as valuable, participants suggested several improvements. Some felt that creating more dynamic movements such as bending down or picking up items from the floor could enhance the experience, making it even more relatable. Moreover, visual guidance on location of objects or steps in tasks could alleviate some of the confusion and frustration, making the tasks feel more manageable.
Many HCPs acknowledged that the simulation deepened their understanding of the challenges faced by dementia patients. This newfound empathy was valuable for novices in the field, as it provided a tangible way to connect with the patient experience. The participants offered several suggestions for enhancing the training experience: providing additional instructions or information during the initial setup could better prepare participants for the tasks ahead; introducing real-world distractions and external interruptions, such as the presence of other people or background noise, could simulate the stress and confusion dementia patients often feel; and incorporating more physical tasks, such as bending or walking, could make the aging suit’s effects even more pronounced and provide a more realistic portrayal of the physical challenges of aging. AREduX provided HCPs with a powerful, immersive way to understand the struggles faced by individuals with dementia. While it was at times frustrating and physically demanding, the overall feedback emphasized that the simulation was a valuable tool for developing empathy and insight into the patient experience. The findings suggest that such simulations could be an essential component of training for both experienced and new healthcare professionals, caregivers, and those involved in elder care, helping them connect more deeply with their patients and better address their needs. The observations from the two caregivers who participated in the AREduX simulation experience share several similarities and differences compared to the experiences of the HCPs. These insights provide a deeper understanding of how caregivers and HCPs respond to the challenges posed by the AREduX scenarios in simulating dementia-related impairments.
Similarities Between Caregivers and HCPs
Both caregivers and HCPs experienced significant frustration while performing the simulated tasks; both identified the difficulty in manipulating utensils or small objects, which mirrors the dexterity challenges that dementia patients may face. One caregiver stated, “This is frustrating” while struggling to pick up items, and similar sentiments were expressed by HCPs, with many reporting frustration at their inability to complete simple tasks such as picking up a pill or aligning a cup. Moreover, both caregivers and HCPs identified the physical and cognitive strain of the simulation.
Caregivers mentioned that the “weight suit” felt heavy on the hands, which made it harder to grip objects. HCPs similarly commented that the suit restricted their movement and made simple tasks feel larger and more difficult. A caregiver observed, “My arm got really really tired. It was heavy,” echoing HCPs’ observations regarding how the aging suit impedes mobility, especially when performing repetitive tasks.
Both caregivers and HCPs displayed a sense of determination to complete the tasks despite the frustration. This persistence mimicked how dementia patients may attempt a task repeatedly, even if they encounter difficulties. One caregiver noted that she “stayed calm throughout” and was “persistent” even when things did not go smoothly; this mirrored HCPs’ determination to complete the simulation, even when things felt increasingly challenging.
Both groups reported experiencing visual distortions or blurriness, which mimicked the sensory challenges faced by dementia patients, particularly those with visual impairments. A caregiver mentioned, “I had visual gap, like it would get blurry and stuff,” while HCPs also commented on how visual impairments made simple tasks feel more frustrating and confusing.
Differences Between Caregivers and HCPs
None of the participants had any prior experience with AR. Caregivers, especially those with less training in dementia care or AR technology, expressed greater doubt about their ability to complete the simulation tasks. In contrast, HCPs, even those newer to the field, felt the experience was beneficial in building empathy and understanding the frustrations of dementia patients. The caregiver with a personal support worker (PSW) background said, “I don’t know how someone like my PSW would be able to do the AREduX because of language barriers and not enough intelligence,” suggesting that the simulation might be too complex for certain caregivers. HCPs, however, felt the experience would be valuable in training and in empathizing with patients.
Caregivers, especially those with less exposure to AR technology, seemed more frustrated by the technical aspects of the simulation. For example, one caregiver questioned, “What is the circle-y thing that comes and goes on my finger?” showing a level of discomfort with the tech interface. In contrast, HCPs were more comfortable with the technology and felt that, while frustrating, it was part of the process of understanding the dementia experience. HCPs were more focused on how the technology simulated sensory impairments and less distracted by the technical components.
Moreover, caregivers seemed more focused on the physical aspects of the simulation—particularly the heaviness of the aging suit and the strain it placed on their bodies—whereas HCPs were more likely to discuss the emotional and cognitive impact of the experience. For example, while caregivers noted their physical fatigue, HCPs often commented on the emotional fatigue of dealing with the frustration; nonetheless HCPs reported “feeling determined to complete it” and being “proud” of finishing, reflecting their awareness of both the physical and emotional challenges faced by patients.
Caregivers seemed to have less positive experiences with the simulation, with one caregiver remarking, “It seemed like an impossible task.” In contrast, HCPs appeared to see the value in the experience as a learning tool—even if it didn’t perfectly replicate every aspect of dementia—for fostering empathy and a better understanding of dementia care.
In sum, the caregivers’ responses indicated a greater focus on the technical aspects of the simulation and on its authenticity and accessibility, whereas the HCPs were more focused on the emotional and empathy-building aspects. Both groups, however, found the experience to be valuable for understanding the challenges dementia patients face, though caregivers with less training and experience in dementia care or AR technology seemed to have more difficulty engaging with the simulation.
Results
Measures
Empathy. Empathy was measured via the Toronto Empathy Scale (TES; 16-items). The response set employed a 5-point Likert scale, with a range of 0 (never) to 4 (always). Eight items were reverse scored. A mean score was calculated for the overall scale. For this study, the scale demonstrated relatively low reliability (Cronbach’s alpha for pre-simulation TES = .533, for post-simulation TES = .539).
Sense of Competence in Dementia Care. Sense of competence in dementia care was measured via 17 items from the SCIDS scale (Schepers et al., 2012), which included four subscales: professionalism, building relationships, care challenges, and sustaining personhood. The response set used a 4-point Likert scale with a range of 0 (not at all) to 3 (very much). A total score was calculated for the overall scale and each subscale by summing the scores for each item. For this study, the scale demonstrated high reliability overall and moderately high reliability for three of the four subscales (Cronbach’s alpha overall = .896, professionalism subscale = .505, building relationships subscale = .790, care challenges subscale = .765, sustaining personhood subscale = .739).
Statistical Analysis
Statistical analyses were conducted using IBM SPSS Statistics 29. Two data points were imputed for two participants due to a missing response for a single item. Due to the low sample size for caregiver participants, data were first analyzed separately for HCPs and caregivers and then combined for a single group analysis. The internal consistency was assessed via Cronbach’s alpha. A factor analysis was run for the TEQ and produced a single-factor solution with item loadings more than 0.4. Descriptive statistics were run for all variables. Due to the low number of participants, a non-parametric Wilcoxon signed rank test test was conducted to compare median scores (Field, 2018)) for both groups separately and for the combined group. A paired samples t-test (Field, 2018) was run to compare the mean scores of the TES pre-simulation and post-simulation for both groups separately and for the combined group. An independent sample t-test (Field, 2018) was run to compare the mean scores of the TES pre-simulation and post-simulation and the SCIDS post-simulation for the combined group. Statistical significance was determined at p < .05.
Data Descriptives
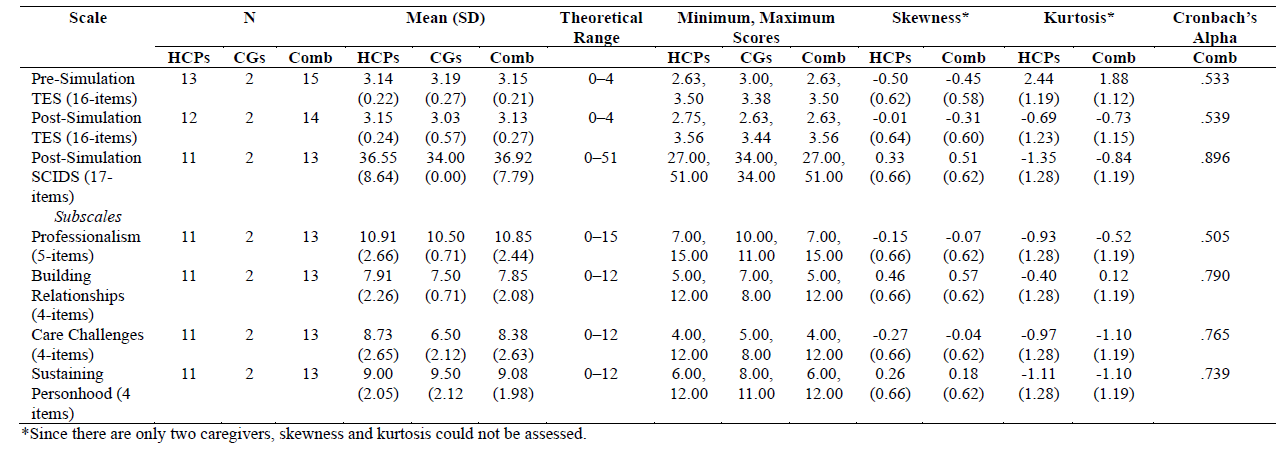
A total of 13 HCPs completed the pre-simulation TEQ and post-simulation TEQ (see Table 1). One HCP did not complete the post-simulation TEQ and two HCPs did not complete the post-simulation SCIDS. The mean and standard deviation for pre-simulation TEQ, post-simulation TEQ, and post-simulation SCIDS are 2.06 (0.17), 2.05 (0.20), and 37.50 (8.48), respectively. The pre-simulation and post-simulation TEQ scores are slightly positively skewed (greater distribution to the left), while the post-simulation SCIDS scores are slightly negatively skewed (greater distribution to the right of the curve), but all are in an acceptable range for skewness. The post-simulation TEQ and SCIDS scores have a slightly flattened curve (platykurtic) and are within the acceptable range (less than 2). The pre-simulation TEQ scores have a peaked curve (leptokurtic) and are just above the acceptable range (more than 2).
Two caregivers completed the pre-simulation and post-simulation (see Table 1). The mean and standard deviation for pre-simulation TEQ, post-simulation TEQ, and post-simulation SCIDS are 3.19 (0.27), 3.03 (0.57), and 34.00 (0.00), respectively. Since there are only two caregivers, skewness and kurtosis could not be assessed.
In the combined dataset, a total of 13 HCPs and 2 caregivers completed the pre-simulation TEQ and post-simulation TEQ. One HCP did not complete the post-simulation TEQ and two HCPs did not complete the post-simulation SCIDS. The mean and standard deviation for pre-simulation TEQ, post-simulation TEQ, and post-simulation SCIDS are 3.15 (0.21), 3.13 (0.27), and 36.92 (7.79), respectively (see Table 1). The pre-simulation and post-simulation TEQ scores are slightly positively skewed (greater distribution to the left), while the post-simulation SCIDS scores are slightly negatively skewed (greater distribution to the right of the curve), but all are in an acceptable range for skewness. The post-simulation TEQ and SCIDS scores have a slightly flattened curve (platykurtic), and are within the acceptable range (less than 2). The pre-simulation TEQ scores have a peaked curve (leptokurtic) and are just above the acceptable range (more than 2). The internal consistency (Cronbach’s alpha) for the pre-simulation and post-simulation TEQ are relatively low, while the post-simulation SCIDS is at an acceptable level, including for three of the four subscales.
Table 1
Descriptive Statistics for Pre- and Post-Simulation Scores on the TES and SCIDS for Healthcare Professionals (HCPs), Caregivers (CGs), and Combined Datasets (Comb)
Non-Parametric Wilcoxon Signed Rank Test
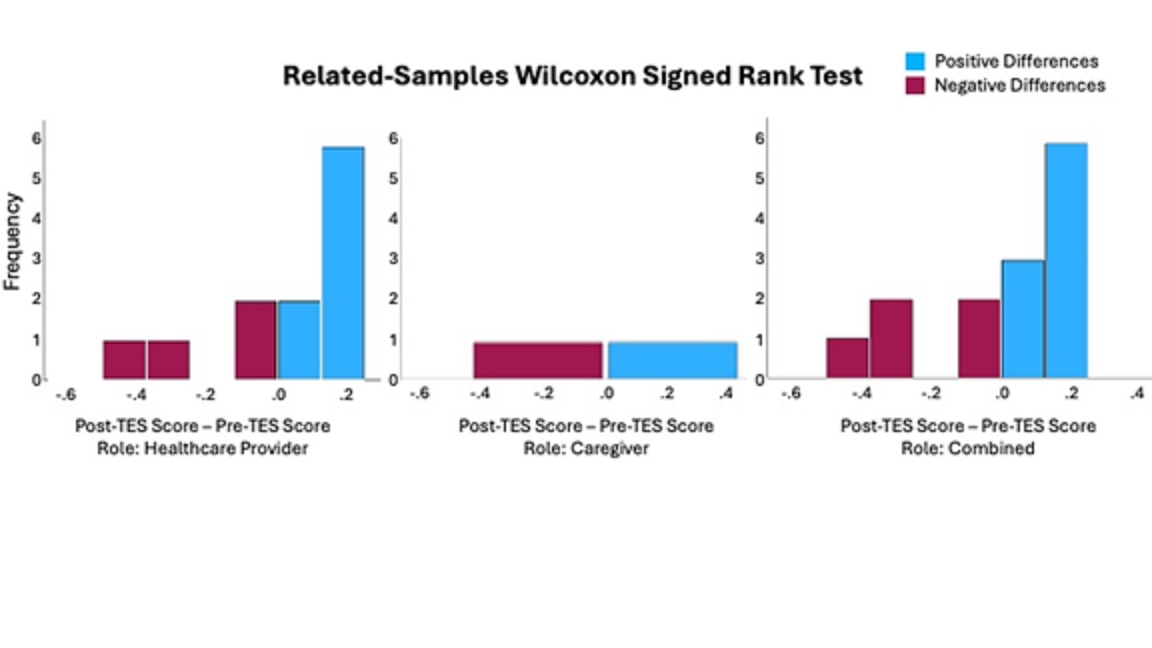
Due to the small number of participants, a non-parametric Wilcoxon signed rank test was conducted. No significant difference was found in empathy levels in the TES before and after the simulation for any of the datasets. The results for each dataset are as follows: HCPs, before (median = 2.13) and after (median = 2.06), T = 41.00, p = .474, r = 0.10; Caregivers, before (median = 3.19) and after (median = 3.03), T = 1.00, p = .655, r = -0.32; combined, before (median = 3.13) and after (median = 3.19), T = 50.00, p = .752, r = 0.08 (see Table 2 and Figure 4).
Table 2
Results of Wilcoxon Signed Rank Test Comparing Scores on the TES Pre- and Post-Simulation for HCPs.
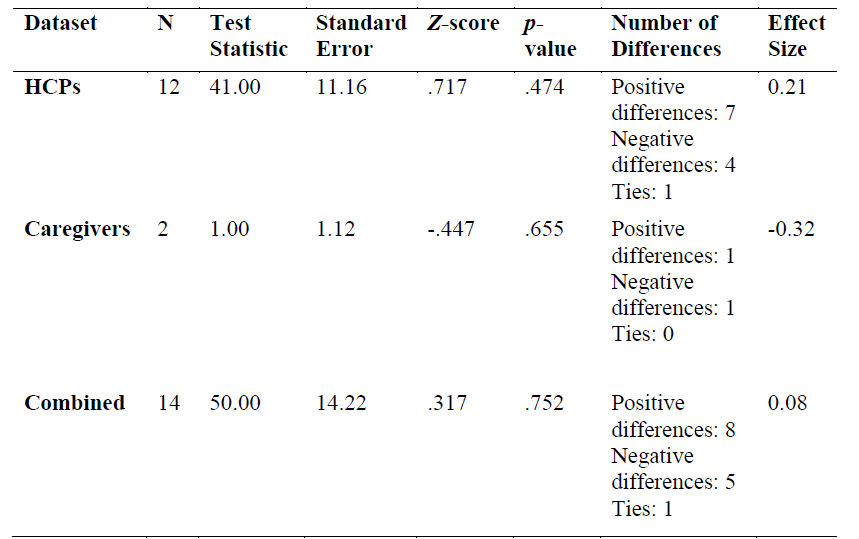
Hypothesis0: There is no difference in the median between the mean score of pre-simulation TES and mean score of post-simulation TES.
Figure 4
Frequency of Pre- and Post-Simulation Scores on the TES
T-Test
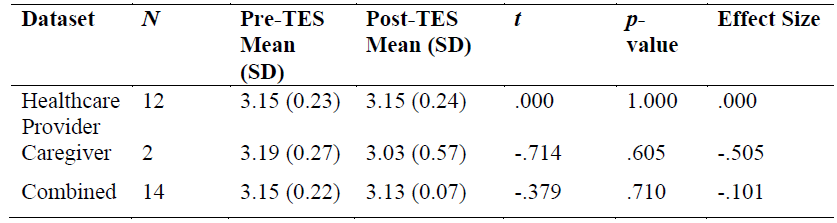
In a paired samples t-test, no significant difference was found in the mean scores for the TES before and after the simulation for HCPs, caregivers, or the combined dataset (see Table 3).
Table 3
Results of Paired Samples t-tests Comparing Scores on the TES Pre- and Post-Simulation for HCPs, Family Caregivers, and Combined Datasets.
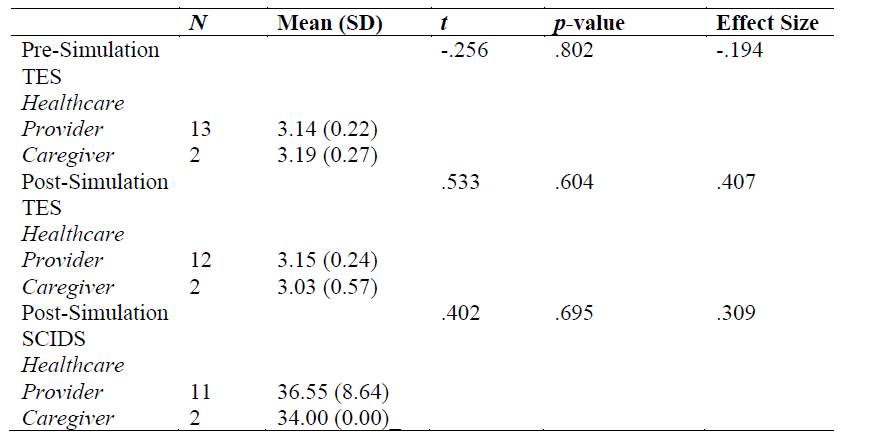
When comparing HCPs and caregivers in an independent samples t-test, there is no significant difference in the pre-simulation TES, post-simulation TES, and post-simulation SCIDS (see Table 4).
Table 4
Results from Independent Samples t-tests Comparing HCPs Versus Family Caregivers on Pre- and Post-Simulation Scores on the TES and the SCIDS.
Qualitative Analysis of Focus Group Results
Transcriptions of the focus-group sessions were analyzed qualitatively using an open-coding process which enabled identification of themes within the data. The analysis was accomplished using the Nvivo qualitative data-analysis software. The identified themes are detailed below.
Theme 1: Description of what happened during the experience. This theme includes descriptions of what participants saw and did while using AREduX, as well as any thoughts, reactions, and feelings they had during the experience. Participants described seeing objects in front of them, attempting to pick them up, and having difficulty grasping them; some noted blurry vision and problems with depth perception. To a limited extent, aspects of the experience were described as interesting and fun, but most comments indicated that aspects of the experience were difficult and frustrating.
Theme 2: General comments about the overall experience. This theme comprises comments regarding general aspects of the experience, as opposed to specific elements. The majority of comments about AREduX are positive. More specifically, participants mentioned that it was exciting, interesting, fun, and valuable. Many participants also noted, however, that the experience was challenging. Most thought it was realistic whereby their experiences mimicked what we believe PLWD experience. Yet, one participant did not believe the experience reflected the life of a PLWD, partly because it is not possible to truly know what they experience. There were also comments on the use of AR, which participants thought substantially added to the experience. For most participants, it was their first experience with AR.
Theme 3: Suggestions for future use. This theme includes suggestions for how AREduX could be used in the future for education or training, and how it could be improved upon and expanded. Participants thought that AREduX would be useful for students and HCPs who are new to working with PLWD and for family members of people recently diagnosed with dementia. At the other end of the experience spectrum, participants thought that AREduX would be useful for experienced HCPs who may have become desensitized over time to the experiences of PLWD; in this situation, AREduX could be used to “refresh empathy” and to remind HCPs of what PLWD are going through.
The suggestions for improvements focus on preparation before and debriefing after the experience, as well as on ideas for expansion of AREduX. Ten participants agreed that they would have benefitted from an idea of what to expect, better instructions, and more preparation. They also thought that an explanation, debriefing, and opportunity for discussion could be provided after they completed the simulation, which would clarify and reinforce the experience and contextualize it within the dementia framework.
Suggestions for expansion of the experience include extending the duration via inclusion of additional scenarios and increasing the intensity of the experience by incorporating additional noises and/or visual distortions. Furthermore, participants thought it would be useful for HCPs to repeat the experience on a regular basis, with added variety in the scenario(s).
Theme 4. Insights gained and impact of participating in AREduX. This theme includes any mention of increased understanding or appreciation of the difficulties that PLWD may experience. Most participants thought their engagement with AREduX provided them with a better understanding of the perspective and difficulties of PLWD. Some noted that this will impact the future care they provide. Most indicated that their empathy for PLWD increased, although some reported no change in this regard.
Theme 5. Equipment not working. This theme includes observations of technical difficulties and uncertainty about whether apparent equipment malfunctions were intended features of AREduX. Most participants noted technical problems with AREduX. More specifically, they found various unintentional “glitches” frustrating and felt that they detracted from the experience. There was uncertainty about whether some of the glitches were intentional (e.g., the display freezing or objects appearing to float). Participants expressed concern that they may have somehow been responsible for the technical difficulties; further, they noted that their experience would have been better and more immersive if they had known whether the problems were caused by themselves or by malfunctioning equipment, or if they were intentional features of AREduX (such as the intentional difficulty in picking things up).
Theme 6. Aging suit. This theme is composed of any mention of the aging suit. Participants appreciated the suit and thought that it complemented the AR part of the experience well. They thought that the physical stress and restriction they experienced while wearing the suit provided them a better understanding of the everyday lives of PLWD. Participants noted that that the suit was heavy and felt heavier after wearing it for a while.
The AREduX simulation experience offers a novel approach to dementia-care education through AR, addressing a growing need for empathy-driven training among HCPs and caregivers. Despite the lack of a statistically significant change in pre- and post-simulation empathy scores on the Toronto Empathy Questionnaire (TEQ), the qualitative data demonstrate a marked affective impact on participants. Focus-group-session feedback highlighted powerful emotional responses, including frustration, fatigue, and cognitive overload—emotions commonly associated with the lived experience of PLWD. These rich qualitative insights affirm that AREduX fosters empathy and deepens understanding of dementia in ways not easily measured by conventional tools.
These emotional responses indicate that AREduX succeeded in creating an embodied experience, even if standard self-report tools such as the TEQ failed to fully capture the change. This discrepancy highlights a limitation of traditional empathy metrics in measuring the short-term, situational, or affective shifts that immersive experiences like AREduX are designed to provoke. Further, increased scores on the SCIDS scale suggest that even when empathy measures remain static, confidence in providing care may still be enhanced through experiential learning.
Participants described the experience as realistic and immersive, especially when the AR component was combined with the physical constraints imposed by the aging suit. Tasks such as setting a table or taking medication, which were intentionally made more difficult, fostered an appreciation for the frustration and fatigue experienced by PLWD. Interestingly, HCPs with greater clinical exposure were more likely to reflect on emotional fatigue and implications for care, while caregivers focused more on physical challenges and usability. This difference underscores the value of tailoring simulation content and delivery to specific learner contexts.
Although most participants were supportive of AREduX as a learning tool, several technical and structural limitations emerged. Technical issues, including software-based glitches and unclear interface functions, interrupted immersion and caused uncertainty about whether perceived impairments were real or simulated. Additionally, some participants lacked adequate preparation for what to expect from the simulation, suggesting that a more structured pre-brief, as well as a debriefing process that provides participants with an opportunity to reflect upon their experience and embody dementia symptoms, is essential to maximize the educational value of the tool.
The findings from this study offer important insights into the experiential impact of AREduX. While quantitative data from the TEQ did not yield statistically significant changes in empathy levels post-simulation, qualitative feedback suggests that participants experienced a strong emotional and cognitive response to the intervention. This divergence illustrates a critical consideration in empathy research: it highlights that standardized self-report tools may fail to fully capture nuanced or context-dependent changes in empathic understanding, especially over short timeframes. Participants described the simulation as immersive, meaningful, and at times frustrating, accurately reflecting the intended experiential design to simulate physical and cognitive challenges associated with dementia.
Frustration related to visual impairments, restricted movement, and difficulty with object manipulation was consistently reported and interpreted by participants as insightful, deepening their appreciation for the everyday struggles of PLWD. This suggests that while quantitative shifts were modest, the simulation successfully evoked affective empathy, which is a crucial step toward behavioural change in care practices.
The SCIDS scores, which assess participants’ sense of competence in dementia care, indicated relatively enhanced post-simulation confidence levels among HCPs and caregivers. These findings underscore the value of combining immersive educational tools with structured learning outcomes, especially when the aim is not only to foster empathy but to reinforce practical caregiving skills.
However, there are several limitations to this study. Technical issues during the simulation disrupted immersion for some participants. Furthermore, participants emphasized the need for structured pre-briefing and debriefing to enhance the simulation’s effectiveness and contextualize the experience. The small sample size of family caregivers limits the statistical power and generalizability of the findings. Moreover, the low internal consistency of the TEQ in this sample may have weakened the sensitivity of the tool to detect subtle or early-stage empathy shifts.
Moreover, the lack of a control group limited causal inferences about the effectiveness of AREduX compared to traditional training methods. Future studies should incorporate randomized controlled designs to strengthen the evidence base.Despite the overall modest scores on empathy measures such as the TEQ, the rich qualitative data reveal significant emotional responses—especially among family caregivers—suggesting that AREduX may better foster affective empathy than cognitive empathy, at least in the short term. Additionally, findings from the NASA-TLX workload index from Phase 2 indicate moderate cognitive demand with areas of elevated frustration, especially among HCPs, indicating the need for more intuitive design and clearer expectations (Hollaender et al. 2023).
This study reaffirms the complexity of measuring empathy development through technology-mediated simulation. Traditional metrics may not capture the full impact of embodied experiences, and empathy changes may take longer to manifest than immediate post-tests can reveal. Nonetheless, the tool’s ability to provoke deep emotional reflection signals its potential as a transformative educational intervention.
Moreover, the lack of a control group limited causal inferences about the effectiveness of AREduX compared to traditional training methods. Future studies should incorporate randomized controlled designs to strengthen the evidence base.Despite the overall modest scores on empathy measures such as the TEQ, the rich qualitative data reveal significant emotional responses—especially among family caregivers—suggesting that AREduX may better foster affective empathy than cognitive empathy, at least in the short term. Additionally, findings from the NASA-TLX workload index from Phase 2 indicate moderate cognitive demand with areas of elevated frustration, especially among HCPs, indicating the need for more intuitive design and clearer expectations (Hollaender et al. 2023).
This study reaffirms the complexity of measuring empathy development through technology-mediated simulation. Traditional metrics may not capture the full impact of embodied experiences, and empathy changes may take longer to manifest than immediate post-tests can reveal. Nonetheless, the tool’s ability to provoke deep emotional reflection signals its potential as a transformative educational intervention.
Future Recommendations
Future studies should consider creating a structured training phase to effectively introduce participants to the AR simulation and its user interface to ensure participants are familiar with the platform’s features, including how to navigate the simulation, interact with key elements, and fully utilize its capabilities. By providing step-by-step instructions and hands-on practice, the training phase could enhance user confidence and ease of use; this would ensure that participants are able to engage with the simulation without technical distractions and allow them to focus on the educational objectives. Enhancing technical robustness by addressing AR hardware glitches and clearly differentiating between simulated impairments and actual errors could also improve user immersion and reduce participant confusion.
The simulation protocol may also benefit from increased variety; creating multiple scenarios and increasing participants’ exposure time may serve to deepen understanding, maintain engagement, and accommodate repeated use for long-term empathy reinforcement.
Additionally, future researchers should consider refining the empathy-measurement approach by embedding alternative or supplemental empathy-measurement tools with higher reliability and sensitivity, such as observational methods, behavioral assessments, or mixed-method diaries.
Finally, future studies might consider scaling up. More specifically, the sample size could be increased, as larger and diverse participant pools will improve statistical power and enable subgroup analysis, such as comparing novice and experienced HCPs and/or formal and informal caregivers. Longitudinal tracking studies at one- and three-month intervals could be conducted to assess whether increases in empathy or care competence are retained over time. The institutional integration of AREduX into existing professional development, university curricula, and caregiver support programs to support wide-scale adoption is another way to scale up.
Conclusion
This study presents the development and early evaluation of AREduX, an AR-based dementia simulation tool designed to foster empathy and care competence among HCPs and caregivers. While quantitative data from the TEQ did not show significant pre- and post-simulation differences, the SCIDS scores demonstrated improvements in perceived care competence. More importantly, valuable qualitative insights revealed that participants experienced frustration, disorientation, and physical strain—emotions that mirror the lived reality of PLWD. Participants reported that the immersive experience was enhanced by the combination of AR and the aging suit and provided a deeper appreciation of the challenges faced by PLWD. These responses suggest that AREduX effectively stimulated empathy, even if the standard TEQ and the SCIDS scale did not detect changes. HCPs reflected more on emotional fatigue and care-practice implications, while caregivers emphasized physical usability and accessibility—underscoring the need to tailor simulation content to distinct learner groups. Despite several technical limitations and a small, non-diverse sample size, the study offers promising evidence for the use of AR in experiential empathy training. Participants expressed strong support for incorporating AREduX into formal education and caregiver-support programs. Suggestions for improving the tool included refining interface usability, expanding scenario diversity, and enhancing structured pre-briefing and debriefing sessions.
Future work will focus on studies with larger and more diverse cohorts, development of more sensitive empathy-assessment tools, and testing of AREduX in varied real-world settings. With continued refinement, AREduX holds considerable potential as a scalable, immersive training platform that can enhance empathy, improve care delivery, and ultimately contribute to better outcomes for PLWD and their caregivers.
AREduX can be integrated into various education environments including the professional development of HCPs; orientation and preparation prior to practicum experiences; and within academic curricula. Our work on the study of empathy has profound implications for understanding the lived experience of groups and populations. Our experience developing AREduX and our study results will inform the development of more targeted approaches for skill development and training to prevent negative outcomes for PLWD and their caregivers. AREduX will provide caregivers training that will enable them to care more effectively for PLWD. Further, the findings from our proposed research program will substantially contribute to the scientific literature on the development of empathy; address the knowledge gap that exists regarding evidence-based understanding of empathy as a construct and its associated dimensions from the perspective of HCPs and caregivers of PLWD; impact how empathy is conceptualized and taught within our curriculum and community; and contribute to guiding further research aligned with implementing AR in experiential education in order to enhance empathy among HCPs and caregivers of PLWD.
References
Alzheimer Society of Canada. (2010a). Navigating the path forward for dementia in Canada. https://alzheimer.ca/sites/default/files/documents/Landmark-Study-Report-1-Path_Alzheimer-Society-Canada_0.pdf
Alzheimer Society of Canada. (2010b). Rising tide: The impact of dementia on Canadian society. https://alzheimer.ca/sites/default/files/documents/Rising-tide_Alzheimer-Society.pdf
Alzheimer Society of Canada. (2024). The many faces of dementia in Canada (Report 2). https://alzheimer.ca/sites/default/files/documents/ASC_The%20Many%20Faces%20of%20Dementia%20In%20Canada_Landmark%20Study_Vol2.pdf
Alzheimer’s Disease International. (2024). World Alzheimer report 2024: Global changes in attitudes to dementia. https://www.alzint.org/u/World-Alzheimer-Report-2024.pdf
Cai, Y., Yang, Y., Ge, Q., & Weng, H. (2023). The interplay between teacher empathy, students’ sense of school belonging, and learning achievement. European Journal of Psychology of Education, 38(3), 1167–1183. https://doi.org/10.1007/s10212-022-00637-6
Canadian Centre for Economic Analysis. (2023). Dementia in Canada: Economic Burden 2020 to 2050. https://www.cancea.ca/wp-content/uploads/2023/07/CANCEA-Economic-Impact-of-Dementia-in-Canada-2023-01-08.pdf
Canadian Nurses Association. (2016). Dementia in Canada: Recommendations to support care for Canada’s aging population. https://hl-prod-ca-oc-download.s3-ca-central-1.amazonaws.com/CNA/2f975e7e-4a40-45ca-863c-5ebf0a138d5e/UploadedImages/documents/Dementia_in_Canada_Recommendations_to_support_care_for_Canadas_aging_population.pdf
Cunico, L., Sartori, R., Marognolli, O., & Meneghini, A. M. (2012). Developing empathy in nursing students: A cohort longitudinal study. Journal of Clinical Nursing, 21(13–14), 2016–2025. https://doi.org/10.1111/j.1365-2702.2012.04105.x
Dal Santo, L., Pohl, S., Saiani, L., & Battistelli, A. (2013). Empathy in the emotional interactions with patients: Is it positive for nurses too? Journal of Nursing Education and Practice, 4(2), 74–81. https://doi.org/10.5430/jnep.v4n2p74
Field, A. P. (2018). Discovering statistics using IBM SPSS statistics: North American edition (5th ed.). SAGE Publications.
Hardy, C. J. D., Marshall, C. R., Golden, H. L., Clark, C. N., Mummery, C. J., Griffiths, T. D. Bamiou, D.-E., & Warren, J. D. (2016). Hearing and dementia. Journal of Neurology, 263, 2339–2354. https://doi.org/10.1007/s00415-016-8208-y
Hojat, M., Maio, V., Pohl, C. A., & Gonnella, J. S. (2023). Clinical empathy: Definition, measurement, correlates, group differences, erosion, enhancement, and healthcare outcomes. Discover Health Systems, 2(1), 8. https://doi.org/10.1007/s44250-023-00020-2
Hollaender, G., Peisachovich, E., Kapralos, B., et al. (2023). Augmented Reality Education Experience (AREduX): An augmented reality experience and experiential education medium to teach empathy to healthcare providers and caregivers of persons living with dementia. Cureus, 15(11), e48384. https://doi.org/10.7759/cureus.48384
Home Care Ontario. (2017). Dementia and home care—Advice on Ontario’s dementia strategy. https://homecareontario.ca/wp-content/uploads/2023/11/dementia-and-home-care-march-2017-home-care-ontario-6.pdf
Jones, P. R., Somoskeöy, T., Chow-Wing-Bom, H., & Crabb, D. P. (2020). Seeing other perspectives: Evaluating the use of virtual and augmented reality to simulate visual impairments (OpenVisSim). NPJ Digital Medicine, 3, 32. https://doi.org/10.1038/s41746-020-0242-6
Julious, S. A. (2005), Sample size of 12 per group rule of thumb for a pilot study. Pharmaceutical Statististics, 4, 287–291. https://doi.org/10.1002/pst.185
Keshtkar, L., Madigan, C. D., Ward, A., Ahmed, S., Tanna, V., Rahman, I., Bostock, J., Nockels, K., Wang, W., Gillies, C. L., & Howick, J. (2024). The effect of practitioner empathy on patient satisfaction. Annals of Internal Medicine, 177(2), 196–209. https://doi.org/10.7326/M23-2168
Kolb, D. A. (1984). Experiential learning: Experience as the source of learning and development. Prentice-Hall.
Peisachovich, E., Kapralos, B., Da Silva, C., Dubrowski, A., Graham, N. L., & Jokel, R. (2022) Focus group findings to support the preliminary development of the Augmented Reality Education Experience (AREduX). Cureus 14(6). e26304. https://doi.org/10.7759/cureus.26304
Prince, M., Bryce, R., Albanese, E., Wimo, A., Ribeiro, W., & Ferri, C. P. (2013). The global prevalence of dementia: A systematic review and meta-analysis. Alzheimer’s and Dementia: The Journal of the Alzheimer’s Association, 9(1), 63–75. https://doi.org/10.1016/j.jalz.2012.11.007
Salazar, K., Adams, J. L., Nies, M. A., Robinson, R., Hedwig, T., & Hellem, T. (2023). Our patients need empathy training across healthcare professions. American Journal of Pharmaceutical Education, 87(5), 100011. https://doi.org/10.1016/j.ajpe.2022.09.001
Sauro, J. (2011). Practical guide to the system usability scale: Background, benchmarks & best practices. CreateSpace Independent Publishing Platform.
Schepers, A. K., Orrell, M., Shanahan, N., & Spector, A. (2012). Sense of competence in dementia care staff (SCIDS) scale: Development, reliability, and validity. International Psychogeriatrics, 24(7), 1153–1162. https://doi.org/10.1017/S104161021100247X
Sinclair, S., Hack, T. F., Raffin-Bouchal, S., McClement, S., Stajduhar, K., Singh, P., Hagen, N., Sinnarajah, A., & Chochinov, H. M. (2018). What are healthcare providers’ understandings and experiences of compassion? The healthcare compassion model: A grounded theory study of healthcare providers in Canada. BMJ Open, 8(3), 1–13. https://doi.org/10.1136/bmjopen-2017-019701
Spreng, R. N., McKinnon, M. C., Mar, R. A., & Levine, B. (2009). The Toronto Empathy Questionnaire: Scale development and initial validation of a factor-analytic solution to multiple empathy measures. Journal of Personality Assessment, 91(1), 62–71. https://doi.org/10.1080/00223890802484381
Winn, B. M. (2009). The design, play, and experience framework. In R. E. Ferdig (Ed.), Handbook of research on effective electronic gaming in education (pp. 1010–1024). IGI Global.
Winter, R., Leanage, N., Roberts, N., Norman, R. I., & Howick, J. (2022). Experiences of empathy training in healthcare: A systematic review of qualitative studies. Patient Education and Counseling, 105(10), 3017–3037. https://doi.org/10.1016/j.pec.2022.06.015
World Health Oganization. (2021). Global status report on the public health response to dementia. https://iris.who.int/server/api/core/bitstreams/9e8aab50-ca34-45e0-9fb0-26e675746f65/content
Zwijsen, S. A., van der Ploeg, E., Hertogh, C. M. P. M. (2016). Understanding the world of dementia. How do people with dementia experience the world? International Psychogeriatrics, 28(7), 1067–1077. https://doi.org/10.1017/S1041610216000351
Author Biographies
Dr Eva Peisachovich, RN PhD
Dr Peisachovich is an associate professor at the School of Nursing at York University, Toronto, Ontario. Her program of research involves exploring, developing, and implementing pedagogies associated with simulation-based environments including human simulation, virtual and augmented reality, serious games, and eLearning approaches to promote professional competence among learners both within higher education milieus and in their transition to the workplace.
Email: peva@yorku.ca
ORCID: 0000-0023-0434-3886
Dr Tin D. Vo
Dr Vo is an assistant professor at the Factor-Inwentash Faculty of Social Work, University of Toronto, Toronto, Canada. Dr. Vo’s equity-focused and interdisciplinary research program explores social exclusion and belonging as determinants of health for historically marginalized communities to shape socially and culturally responsive systems of care.
Email: tin.vo@utoronto.ca
ORCID: https://orcid.org/0000-0002-5909-7789
Dr Bill Kapralo
Dr Bill Kapralos is an associate professor in the Game Development and Interactive Media program at Ontario Tech University. His current research interests include immersive technologies, immersive virtual-learning environments including serious gaming and virtual simulation, multi-modal virtual environments, the perception of auditory events, and 3D (spatial) sound generation.
Email: bill.kapralos@ontariotechu.ca
ORCID: 0000-0003-0434-3847
Dr Celina da Silva, RN, PhD
Dr da Silva is an associate professor, School of Nursing, York University. Her program of research focuses on virtual serious games (VSGs) and simulation-based education in healthcare. She co-led the development of Moirai, an open-source VSG platform, and employs co-design methodologies to create accessible, equity-driven educational tools for internationally educated nurses, caregivers, and healthcare professionals.
Email:celinads@yorku.ca
https://orcid.org/0000-0002-1561-5708
Dr Naida L. Graham, PhD
Dr Graham is a research associate at the School of Nursing at York University, Toronto, Ontario. She is involved in development and evaluation of simulated learning environments for use in empathy training of healthcare providers. Previously, and for the majority of her career, she conducted research on cognitive (especially language) impairments in dementia.
Email: nlg10@yorku.ca
https://orcid.org/0009-0001-3926-2353
Shai Rahmanov
Shai is a graduate of the School of Environmental Studies and Urban Change at York University, with a deep commitment to advancing the role of technology in health and environmental change. As a research assistant on this project, Shai has contributed to exploring how innovative technologies can bridge gaps in healthcare and environmental awareness. His work centres on leveraging the power of immersive technologies to enhance understanding and drive transformative change in these fields. Shai is interested in how immersive technologies can be used to create experiences that encourage sustainable actions and improve health outcomes.




Recent articles
- Index of volume 21 number 221 Jun 2026
- What does Canada’s new National Artificial Intelligence Strategy mean for healthcare?21 Jun 2026
- UN SDGs and Open Source Principles as Outcomes and Implementation Approach to Health Informatics21 Jun 2026
- Designing Compassionate Systems: Why Nursing Must Lead in the Age of AI21 Jun 2026
- Advancing Nursing Informatics Through the Integration of Genomics: Addressing Barriers and Capacity Building in Canadian Healthcare21 Jun 2026